

Comparison of two computer algorithms to identify surgical site infections
- PMID: 22136489
- PMCID: PMC3279712
- DOI: 10.1089/sur.2010.109
Comparison of two computer algorithms to identify surgical site infections
Abstract
Background: Surgical site infections (SSIs), the second most common healthcare-associated infections, increase hospital stay and healthcare costs significantly. Traditional surveillance of SSIs is labor-intensive. Mandatory reporting and new non-payment policies for some SSIs increase the need for efficient and standardized surveillance methods. Computer algorithms using administrative, clinical, and laboratory data collected routinely have shown promise for complementing traditional surveillance.
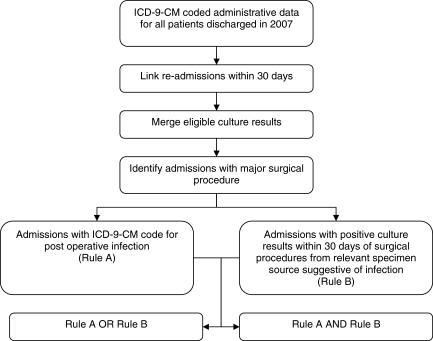
Methods: Two computer algorithms were created to identify SSIs in inpatient admissions to an urban, academic tertiary-care hospital in 2007 using the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM) diagnosis codes (Rule A) and laboratory culture data (Rule B). We calculated the number of SSIs identified by each rule and both rules combined and the percent agreement between the rules. In a subset analysis, the results of the rules were compared with those of traditional surveillance in patients who had undergone coronary artery bypass graft surgery (CABG).
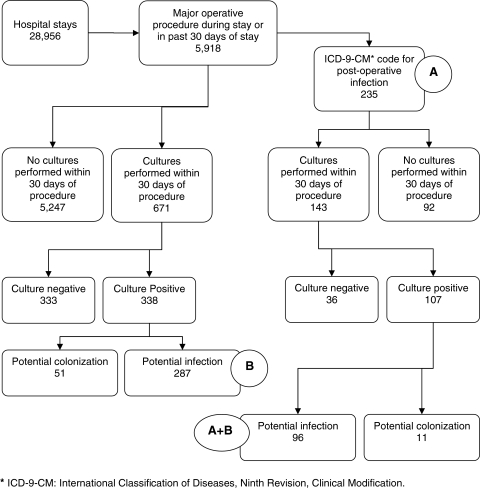
Results: Of the 28,956 index hospital admissions, 5,918 patients (20.4%) had at least one major surgical procedure. Among those and readmissions within 30 days, the ICD-9-CM-only rule identified 235 SSIs, the culture-only rule identified 287 SSIs; combined, the rules identified 426 SSIs, of which 96 were identified by both rules. Positive and negative agreement between the rules was 36.8% and 97.1%, respectively, with a kappa of 0.34 (95% confidence interval [CI] 0.27-0.41). In the subset analysis of patients who underwent CABG, of the 22 SSIs identified by traditional surveillance, Rule A identified 19 (86.4%) and Rule B identified 13 (59.1%) cases. Positive and negative agreement between Rules A and B within these "positive controls" was 81.3% and 50.0% with a kappa of 0.37 (95% CI 0.04-0.70).
Conclusion: Differences in the rates of SSI identified by computer algorithms depend on sources and inherent biases in electronic data. Different algorithms may be appropriate, depending on the purpose of case identification. Further research on the reliability and validity of these algorithms and the impact of changes in reimbursement on clinician practices and electronic reporting is suggested.
Figures
Similar articles
-
Use of Medicare diagnosis and procedure codes to improve detection of surgical site infections following hip arthroplasty, knee arthroplasty, and vascular surgery.Infect Control Hosp Epidemiol. 2012 Jan;33(1):40-9. doi: 10.1086/663207. Epub 2011 Nov 22. Infect Control Hosp Epidemiol. 2012. PMID: 22173521
-
Financial impact of surgical site infections on hospitals: the hospital management perspective.JAMA Surg. 2013 Oct;148(10):907-14. doi: 10.1001/jamasurg.2013.2246. JAMA Surg. 2013. PMID: 23965750
-
Highly sensitive and efficient computer-assisted system for routine surveillance for surgical site infection.Infect Control Hosp Epidemiol. 2006 Aug;27(8):794-801. doi: 10.1086/506393. Epub 2006 Jul 20. Infect Control Hosp Epidemiol. 2006. PMID: 16874638
-
Validity and Reliability of Administrative Coded Data for the Identification of Hospital-Acquired Infections: An Updated Systematic Review with Meta-Analysis and Meta-Regression Analysis.Health Serv Res. 2018 Jun;53(3):1919-1956. doi: 10.1111/1475-6773.12691. Epub 2017 Apr 11. Health Serv Res. 2018. PMID: 28397261 Free PMC article.
-
Selection pressures of vancomycin powder use in spine surgery: a meta-analysis.Spine J. 2019 Jun;19(6):1076-1084. doi: 10.1016/j.spinee.2019.01.002. Epub 2019 Jan 17. Spine J. 2019. PMID: 30660741
Cited by
-
Incidence of Surgical Site Infections and Surgical Antimicrobial Prophylaxis in JNMC, Bhagalpur, India.J Pharm Bioallied Sci. 2022 Jul;14(Suppl 1):S868-S871. doi: 10.4103/jpbs.jpbs_30_22. Epub 2022 Jul 13. J Pharm Bioallied Sci. 2022. PMID: 36110734 Free PMC article.
-
Studies on nurse staffing and health care-associated infection: methodologic challenges and potential solutions.Am J Infect Control. 2015 Jun;43(6):581-8. doi: 10.1016/j.ajic.2015.03.029. Am J Infect Control. 2015. PMID: 26042847 Free PMC article. Review.
-
Electronically assisted surveillance systems of healthcare-associated infections: a systematic review.Euro Surveill. 2020 Jan;25(2):1900321. doi: 10.2807/1560-7917.ES.2020.25.2.1900321. Euro Surveill. 2020. PMID: 31964462 Free PMC article.
-
Incidence and risk factors for and the effect of a program to reduce the incidence of surgical site infection after cardiac surgery.Surg Infect (Larchmt). 2014 Jun;15(3):299-304. doi: 10.1089/sur.2013.048. Epub 2014 May 6. Surg Infect (Larchmt). 2014. PMID: 24800982 Free PMC article.
-
Prevalence and risk factors for antibiotic-resistant community-associated bloodstream infections.J Infect Public Health. 2014 May-Jun;7(3):224-32. doi: 10.1016/j.jiph.2014.01.001. Epub 2014 Mar 13. J Infect Public Health. 2014. PMID: 24631369 Free PMC article.
References
-
- Roy MC. Perl TM. Basics of surgical-site infection surveillance. Infect Control Hosp Epidemiol. 1997;18:659–668. - PubMed
-
- Horan TC. Andrus M. Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36:309–332. - PubMed
-
- Tokars JI. Richards C. Andrus M, et al. The changing face of surveillance for health care-associated infections. Clin Infect Dis. 2004;39:1347–1352. - PubMed
-
- Yokoe DS. Platt R. Surveillance for surgical site infections: The uses of antibiotic exposure. Infect Control Hosp Epidemiol. 1994;15:717–723. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
