

Physiologic partograph to improve birth safety and outcomes among low-risk, nulliparous women with spontaneous labor onset
- PMID: 22138426
- PMCID: PMC3254242
- DOI: 10.1016/j.mehy.2011.11.012
Physiologic partograph to improve birth safety and outcomes among low-risk, nulliparous women with spontaneous labor onset
Abstract
Oxytocin augmentation and cesarean rates among low-risk, term, nulliparous women with a spontaneous onset of labor in the United States approximate 50% and 26.5%, respectively. This indicates that the quality of obstetrical care is less than optimal in this nation. Exorbitant oxytocin use, the intervention most commonly associated with preventable adverse perinatal outcomes, jeopardizes birth safety while the high cesarean rate in this high-volume group compromises population health and increases health care costs. Dystocia, characterized by the slow, abnormal progression of labor, is the most commonly reported indication for primary cesareans, accounting directly for approximately 50% of all nulliparous cesareans and indirectly for most repeat cesareans. Diagnoses of dystocia are most often based on ambiguously defined delays in cervical dilation beyond which labor augmentation is deemed justified. Dystocia is known to be over-diagnosed which undoubtedly contributes to contemporary oxytocin augmentation and primary cesarean rates. Labor attendants would benefit from an evidence-based framework for homogenous labor assessment. To this end, we present a physiologically-based partograph for 'in-hospital' use in assessing the labors of low-risk, term, nulliparous women with spontaneous labor onset. This tool incorporates several evidence-based labor principles that combine to give needed clinical meaning to 'dystocia' as a diagnosis. It is hypothesized that our partograph will safely limit diagnoses of dystocia to only the slowest 10% of low-risk, nulliparous women. This should, in turn, safe-guard against unnecessary, injudicious, and potentially harmful use of oxytocin when labor is already adequately progressing while also indicating when its use may be justified. We further hypothesize that cesareans performed for dystocia in this population will decrease by ≥ 50%. No significant influence on other labor process or labor outcome variables is expected with partograph use. Widespread use of this physiologically-based partograph will be warranted if our hypotheses are supported.
Copyright © 2011 Elsevier Ltd. All rights reserved.
Figures
- ■
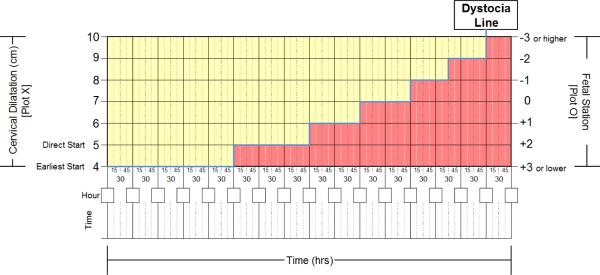
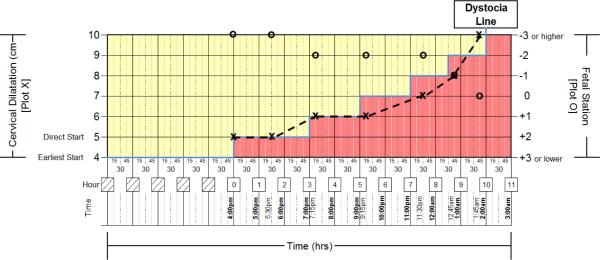
At 9:37 am, the cervix is dilated 5 cm and the fetal head is at −2 station. The partograph is initiated by plotting an `X' at 5 cm on the dystocia line and an `O' at −2 station. On the time line, 9:30 am is documented which becomes the start of hour zero (`0'). The time line is completed in 1-hour increments from that point forward.
- ■
At 12:03 pm, the cervix is dilated 6 cm and the fetal head is at −2 station. Labor progress is adequate, remaining left of the dystocia line and without delay.
- ■
At 2:25 pm, the cervix is dilated 8 cm and the fetal head is at 0 station. Labor progress is adequate, remaining left of the dystocia line and without delay.
- ■
At 4:40 pm, the cervix is completely dilated and the fetal head is at +1 station. Use of the partograph is complete. Second stage labor is managed in the `usual care' pattern of the labor care provider.
- ■
At 4:07 pm, the cervix is dilated 5 cm and the fetal head is at −3 station. The partograph is initiated by plotting an `X' at 5 cm on the dystocia line and an `O' at −3 station. On the time line, 4:00 pm is documented which becomes the start of hour zero (`0'). The time line is completed in 1-hour increments from that point forward.
- ■
At 5:41 pm, the cervix is dilated 5 cm and the fetus head is at −3 station. Labor remains left of the dystocia line without partograph-defined delay.
- ■
At 7:15 pm, the cervix is dilated 6 cm and the fetal head is at −2 station. Labor progress is adequate, remaining left of the dystocia line and without delay.
- ■
At 9:20 pm, the cervix is dilated 6 cm and the fetal head is at −2 station. Labor dystocia is diagnosed as progress moves right of the dystocia line. Thorough assessment is indicated with management option choices including supportive therapy only, oxytocin augmentation, or delivery. Oxytocin augmentation is chosen.
- ■
At 11:39 pm, the cervix is dilated 7 cm and the fetal head is at −2 station. Labor remains right of the dystocia line.
- ■
At 12:52 am, the cervix is dilated 8 cm and the fetal head is at −1 station. Labor remains right of the dystocia line.
- ■
At 1:50 am, the cervix is completely dilated and the fetus is at 0 station. Use of the partograph is complete. Second stage labor is managed in the `usual care' pattern of the labor care provider.
- ■
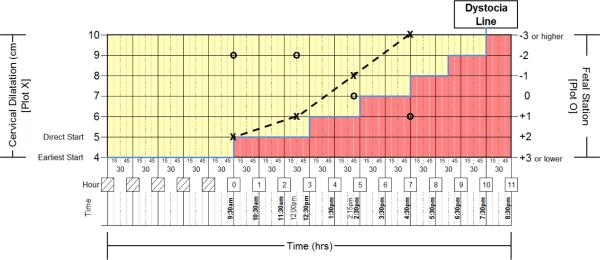
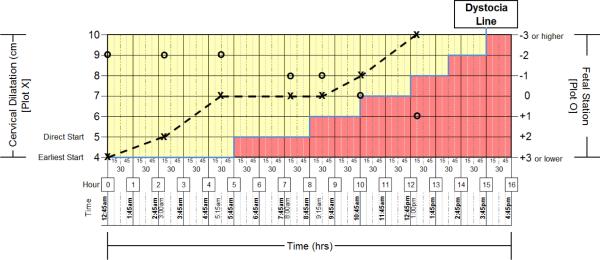
At 11:15 pm, the cervix is dilated 3 cm and the fetal head is at −2 station. The parturient does not yet meet criteria for partograph initiation.
- ■
At 12:54 am, the cervix is dilated 4 cm and fetal head remains at −2 station. The partograph is initiated due to ≥ 1 cm change in dilation in ≤ 2 hour window. An `X' is plotted at 4 cm on the dystocia line and an `O' is plotted at −2 station. On the time line, 12:45 am is documented which becomes the start of hour zero (`0'). The time line is completed in 1-hour increments from that point forward.
- ■
At 3:06 am, the cervix is dilated 5 cm and the fetal head is at −2 station. Labor progress is adequate, remaining left of the dystocia line and without delay.
- ■
At 5:19 am, the cervix is dilated 7 cm and the fetal head is at −2 station. Labor progress is adequate, remaining left of the dystocia line and without delay.
- ■
At 8:10 am, the cervix is dilated 7 cm and the fetal head is at −1 station. Labor remains left of the dystocia line without partograph-defined delay.
- ■
At 9:22 am, the cervix is dilated 7 cm and the fetal head is at −1 station. Labor progress is delayed due to the > 4 hour delay in cervical change. Thorough assessment is indicated with management option choices including supportive therapy only, oxytocin augmentation, or delivery. Oxytocin augmentation is chosen.
- ■
At 10:52 am, the cervix is dilated 8 cm and the fetal head is at 0 station. Labor progress is again adequate, remaining left of the dystocia line.
- ■
At 1:02 pm, the cervix is completely dilated and the fetal head is at +1 station. Use of the partograph is complete. Second stage labor is managed in the `usual care' pattern of the labor care provider.
Similar articles
-
Applying a physiologic partograph to Consortium on Safe Labor data to identify opportunities for safely decreasing cesarean births among nulliparous women.Birth. 2018 Dec;45(4):358-367. doi: 10.1111/birt.12358. Epub 2018 May 30. Birth. 2018. PMID: 29851163 Free PMC article.
-
Pilot Study of Physiologic Partograph Use Among Low-Risk, Nulliparous Women With Spontaneous Labor Onset.J Midwifery Womens Health. 2016 Mar-Apr;61(2):235-41. doi: 10.1111/jmwh.12442. Epub 2016 Feb 24. J Midwifery Womens Health. 2016. PMID: 26917257
-
Labor dystocia and oxytocin augmentation before or after six centimeters cervical dilatation, in nulliparous women with spontaneous labor, in relation to mode of birth.BMC Pregnancy Childbirth. 2022 May 13;22(1):408. doi: 10.1186/s12884-022-04710-2. BMC Pregnancy Childbirth. 2022. PMID: 35562716 Free PMC article.
-
Effect of partograph use on outcomes for women in spontaneous labour at term and their babies.Cochrane Database Syst Rev. 2018 Aug 6;8(8):CD005461. doi: 10.1002/14651858.CD005461.pub5. Cochrane Database Syst Rev. 2018. PMID: 30080256 Free PMC article.
-
Labor Dystocia: A Common Approach to Diagnosis.J Midwifery Womens Health. 2015 Sep-Oct;60(5):499-509. doi: 10.1111/jmwh.12360. J Midwifery Womens Health. 2015. PMID: 26461189 Review.
Cited by
-
Labour admission assessment results of index pregnancy as predictors of intrapartum stillbirth in public health facilities of Addis Ababa: A case-control study.PLoS One. 2020 Apr 2;15(4):e0230478. doi: 10.1371/journal.pone.0230478. eCollection 2020. PLoS One. 2020. PMID: 32240197 Free PMC article.
-
Applying a physiologic partograph to Consortium on Safe Labor data to identify opportunities for safely decreasing cesarean births among nulliparous women.Birth. 2018 Dec;45(4):358-367. doi: 10.1111/birt.12358. Epub 2018 May 30. Birth. 2018. PMID: 29851163 Free PMC article.
-
An Algorithm (LaD) for Monitoring Childbirth in Settings Where Tracking All Parameters in the World Health Organization Partograph Is Not Feasible: Design and Expert Validation.JMIR Med Inform. 2021 May 27;9(5):e17056. doi: 10.2196/17056. JMIR Med Inform. 2021. PMID: 34042599 Free PMC article.
-
Study protocol: the Labor Progression Study, LAPS - does the use of a dynamic progression guideline in labor reduce the rate of intrapartum cesarean sections in nulliparous women? A multicenter, cluster randomized trial in Norway.BMC Pregnancy Childbirth. 2017 Nov 13;17(1):370. doi: 10.1186/s12884-017-1553-8. BMC Pregnancy Childbirth. 2017. PMID: 29132336 Free PMC article. Clinical Trial.
-
Cervical dilatation over time is a poor predictor of severe adverse birth outcomes: a diagnostic accuracy study.BJOG. 2018 Jul;125(8):991-1000. doi: 10.1111/1471-0528.15205. Epub 2018 Apr 17. BJOG. 2018. PMID: 29498187 Free PMC article.
References
-
- Bailit JL, Dierker L, Blanchard MH, Mercer BM. Outcomes of women presenting in active versus latent phase of spontaneous labor. Obstet Gynecol. 2005;105(1):77–79. - PubMed
-
- Holmes P, Oppenheimer LW, Wen SW. The relationship between cervical dilatation at initial presentation in labour and subsequent intervention. BJOG. 2001;108(11):1120–1124. - PubMed
-
- Impey L, Hobson J, O'Herlihy C. Graphic analysis of actively managed labor: prospective computation of labor progress in 500 consecutive nulliparous women in spontaneous labor at term. Am J Obstet Gynecol. 2000;183(2):438–443. - PubMed
-
- Rahnama P, Ziaei S, Faghihzadeh S. Impact of early admission in labor on method of delivery. Int J Gynaecol Obstet. 2006;92(3):217–220. - PubMed
-
- Mikolajczyk R, Zhang J, Chan L, Grewal J. Early versus late admission to labor/delivery, labor progress and risk of caesarean section in nulliparous women. Am J Obstet Gynecol. 2008;199(6 Suppl A):S49.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
