

Adaptive radiotherapy for head-and-neck cancer: initial clinical outcomes from a prospective trial
- PMID: 22138459
- PMCID: PMC4271827
- DOI: 10.1016/j.ijrobp.2011.08.017
Adaptive radiotherapy for head-and-neck cancer: initial clinical outcomes from a prospective trial
Abstract
Purpose: To present pilot toxicity and survival outcomes for a prospective trial investigating adaptive radiotherapy (ART) for oropharyngeal squamous cell carcinoma.
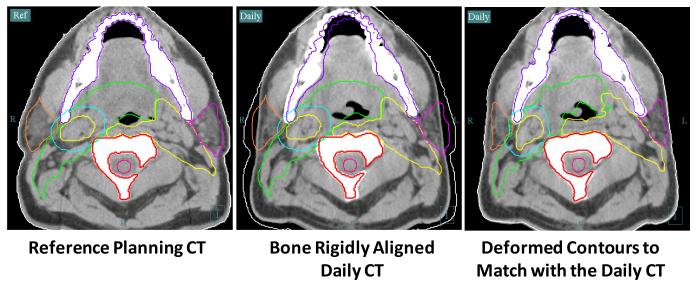
Methods and materials: A total of 24 patients were enrolled in an institutional review board-approved clinical trial; data for 22 of these patients were analyzed. Daily CT-guided setup and deformable image registration permitted serial mapping of clinical target volumes and avoidance structures for ART planning. Primary site was base of tongue in 15 patients, tonsil in 6 patient, and glossopharyngeal sulcus in 1 patient. Twenty patients (91%) had American Joint Committee on Cancer (AJCC) Stage IV disease. T stage distribution was 2 T1, 12 T2, 3 T3, 5 T4. N stage distribution was 1 N0, 2 N1, 5 N2a, 12 N2b, and 2 N2c. Of the patients, 21 (95%) received systemic therapy.
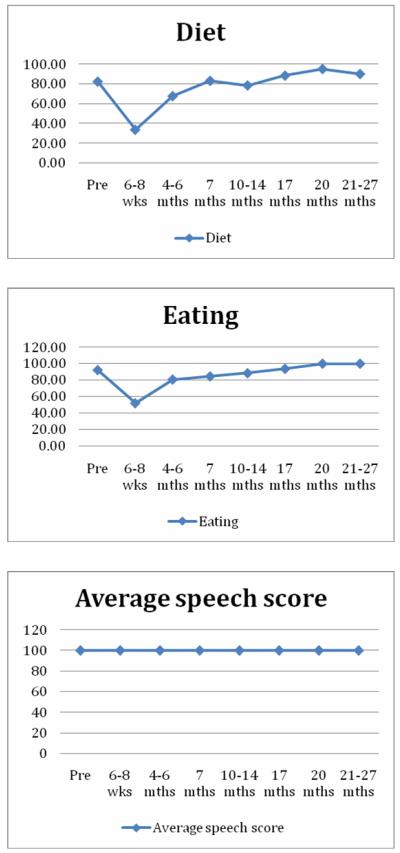
Results: With a 31-month median follow-up (range, 13-45 months), there has been no primary site failure and 1 nodal relapse, yielding 100% local and 95% regional disease control at 2 years. Baseline tumor size correlated with absolute volumetric treatment response (p = 0.018). Parotid volumetric change correlated with duration of feeding tube placement (p = 0.025). Acute toxicity was comparable to that observed with conventional intensity-modulated radiotherapy (IMRT). Chronic toxicity and functional outcomes beyond 1 year were tabulated.
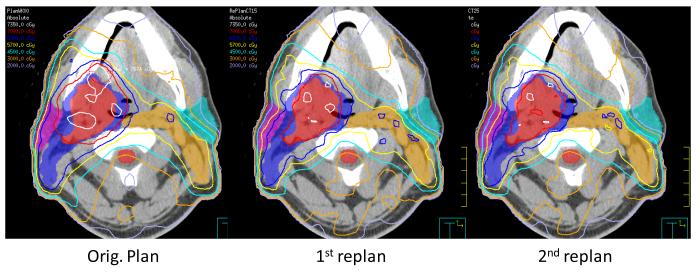
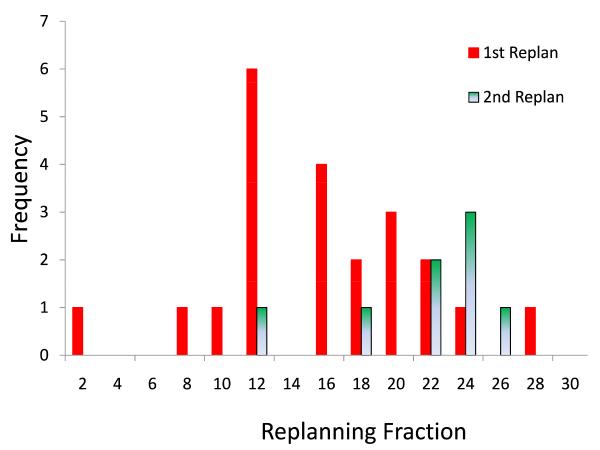
Conclusion: This is the first prospective evaluation of morbidity and survival outcomes in patients with locally advanced head-and-neck cancer treated with automated adaptive replanning. ART can provide dosimetric benefit with only one or two mid-treatment replanning events. Our preliminary clinical outcomes document functional recovery and preservation of disease control at 1-year follow-up and beyond.
Copyright © 2012 Elsevier Inc. All rights reserved.
Figures
References
-
- de Arruda FF, Puri DR, Zhung J, Narayana A, Wolden S, Hunt M, et al. Intensity-modulated radiation therapy for the treatment of oropharyngeal carcinoma: the Memorial Sloan-Kettering Cancer Center experience. Int J Radiat Oncol Biol Phys. 2006 Feb 1;64(2):363–73. - PubMed
-
- Feng FY, Kim HM, Lyden TH, Haxer MJ, Feng M, Worden FP, et al. Intensity-modulated radiotherapy of head and neck cancer aiming to reduce dysphagia: early dose-effect relationships for the swallowing structures. Int J Radiat Oncol Biol Phys. 2007 Aug 1;68(5):1289–98. - PubMed
-
- Yao M, Karnell LH, Funk GF, Lu H, Dornfeld K, Buatti JM. Health-related quality-of-life outcomes following IMRT versus conventional radiotherapy for oropharyngeal squamous cell carcinoma. Int J Radiat Oncol Biol Phys. 2007 Dec 1;69(5):1354–60. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
