

Adoptive immunotherapy with unselected or EBV-specific T cells for biopsy-proven EBV+ lymphomas after allogeneic hematopoietic cell transplantation
- PMID: 22138512
- PMCID: PMC3311278
- DOI: 10.1182/blood-2011-08-371971
Adoptive immunotherapy with unselected or EBV-specific T cells for biopsy-proven EBV+ lymphomas after allogeneic hematopoietic cell transplantation
Abstract
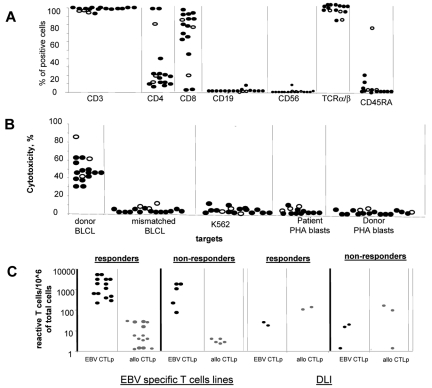
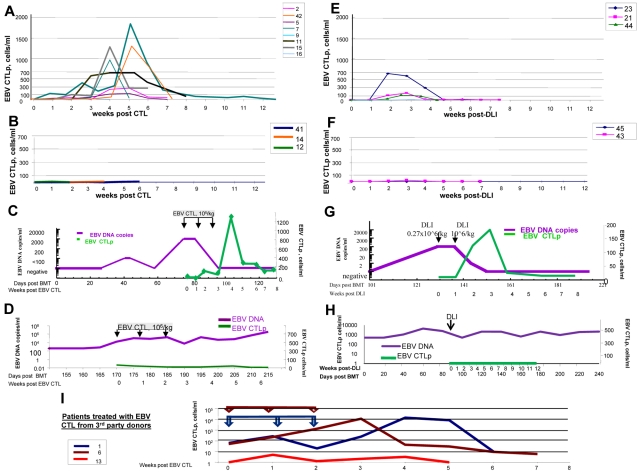
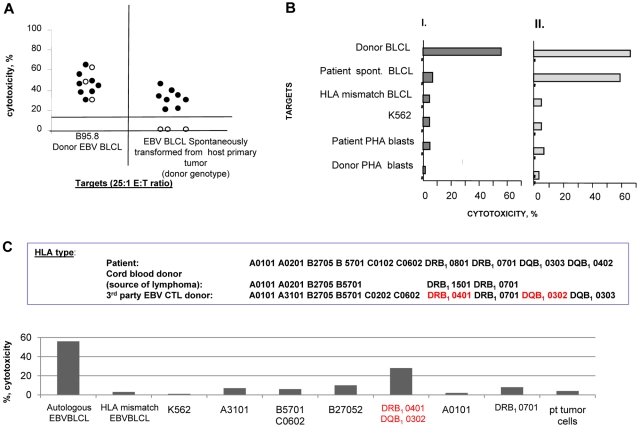
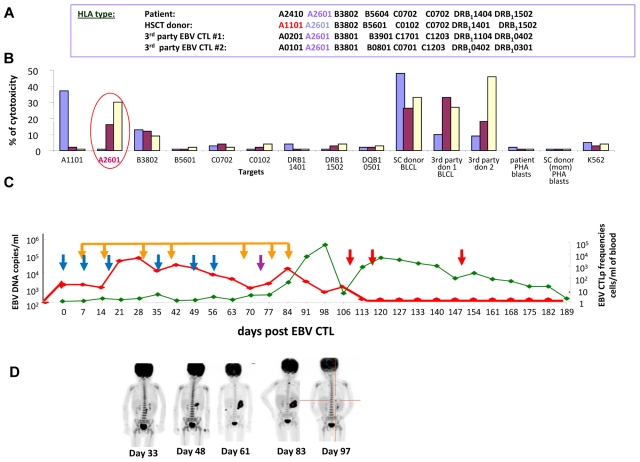
We evaluated HLA-compatible donor leukocyte infusions (DLIs) and HLA-compatible or HLA-disparate EBV-specific T cells (EBV-CTLs) in 49 hematopoietic cell transplantation recipients with biopsy-proven EBV-lymphoproliferative disease (EBV-LPD). DLIs and EBV-CTLs each induced durable complete or partial remissions in 73% and 68% of treated patients including 74% and 72% of patients surviving ≥ 8 days after infusion, respectively. Reversible acute GVHD occurred in recipients of DLIs (17%) but not EBV-CTLs. The probability of complete response was significantly lower among patients with multiorgan involvement. In responders, DLIs and EBV-CTLs regularly induced exponential increases in EBV-specific CTL precursor (EBV-CTLp) frequencies within 7-14 days, with subsequent clearance of EBV viremia and resolution of disease. In nonresponders, EBV-CTLps did not increase and EBV viremia persisted. Treatment failures were correlated with impaired T-cell recognition of tumor targets. Either donor-derived EBV-CTLs that had been sensitized with autologous BLCLs transformed by EBV strain B95.8 could not lyse spontaneous donor-derived EBV-transformed BLCLs expanded from the patient's blood or biopsied tumor or they failed to lyse their targets because they were selectively restricted by HLA alleles not shared by the EBV-LPD. Therefore, either unselected DLIs or EBV-specific CTLs can eradicate both untreated and Rituxan-resistant lymphomatous EBV-LPD, with failures ascribable to impaired T-cell recognition of tumor-associated viral antigens or their presenting HLA alleles.
Figures
Comment in
-
Equal-opportunity treatment of EBV-PTLD.Blood. 2012 Mar 15;119(11):2436-8. doi: 10.1182/blood-2012-01-397828. Blood. 2012. PMID: 22422813 No abstract available.
References
-
- Martin PJ, Shulman HM, Schubach WH, et al. Fatal Epstein-Barr-virus-associated proliferation of donor B cells after treatment of acute graft-versus-host disease with a murine anti-T-cell antibody. Ann Intern Med. 1984;101(3):310–315. - PubMed
-
- Lucas KG, Small TN, Heller G, Dupont B, O'Reilly RJ. The development of cellular immunity to Epstein-Barr virus after allogeneic bone marrow transplantation. Blood. 1996;87(6):2594–2603. - PubMed
-
- Meijer E, Cornelissen JJ. Epstein-Barr virus-associated lymphoproliferative disease after allogeneic haematopoietic stem cell transplantation: molecular monitoring and early treatment of high-risk patients. Curr Opin Hematol. 2008;15(6):576–585. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
