

Differential impact of inhibitory and activating Killer Ig-Like Receptors (KIR) on high-risk patients with myeloid and lymphoid malignancies undergoing reduced intensity transplantation from haploidentical related donors
- PMID: 22139069
- PMCID: PMC3629554
- DOI: 10.1038/bmt.2011.181
Differential impact of inhibitory and activating Killer Ig-Like Receptors (KIR) on high-risk patients with myeloid and lymphoid malignancies undergoing reduced intensity transplantation from haploidentical related donors
Abstract
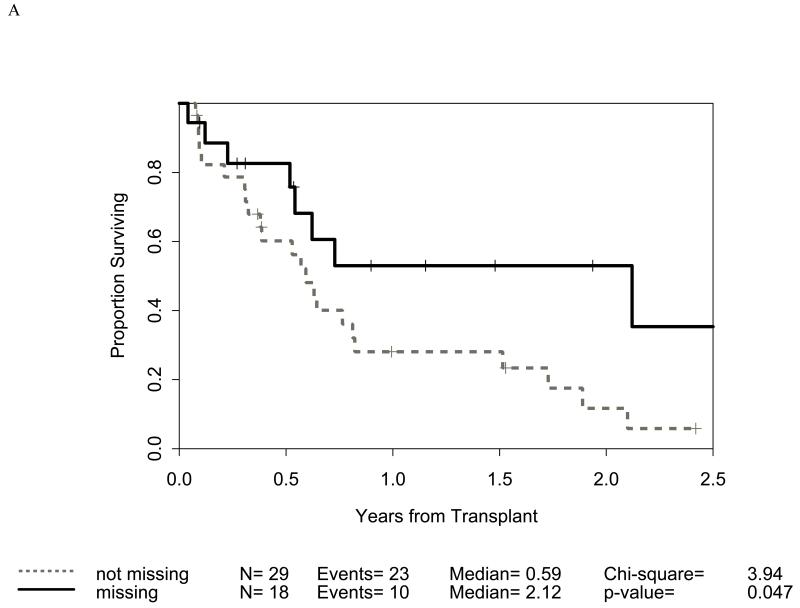
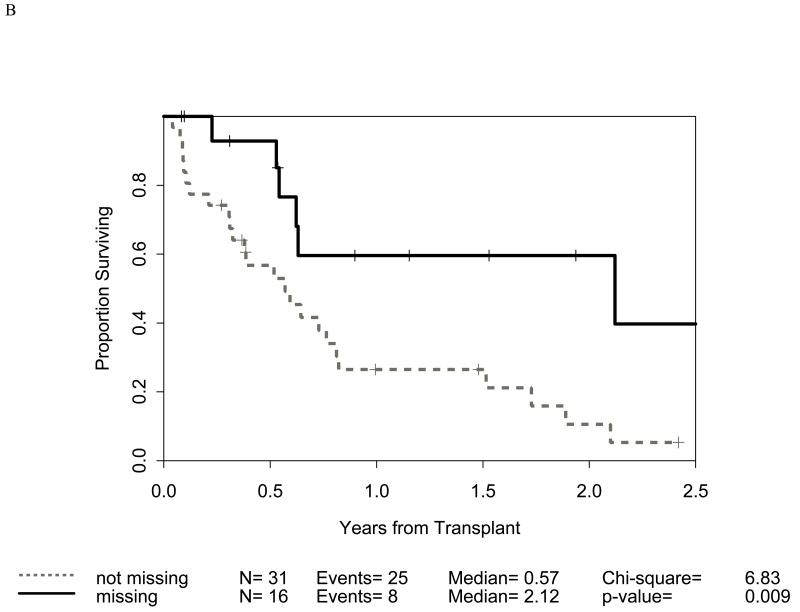
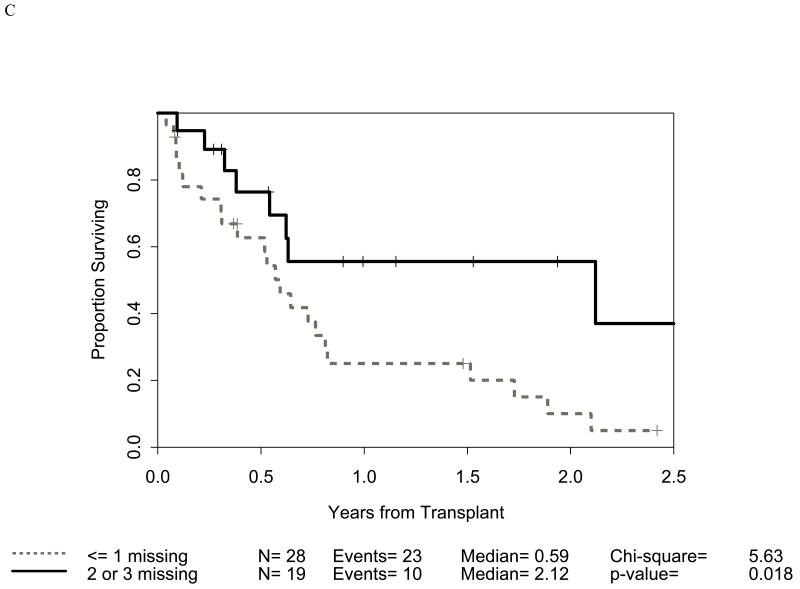
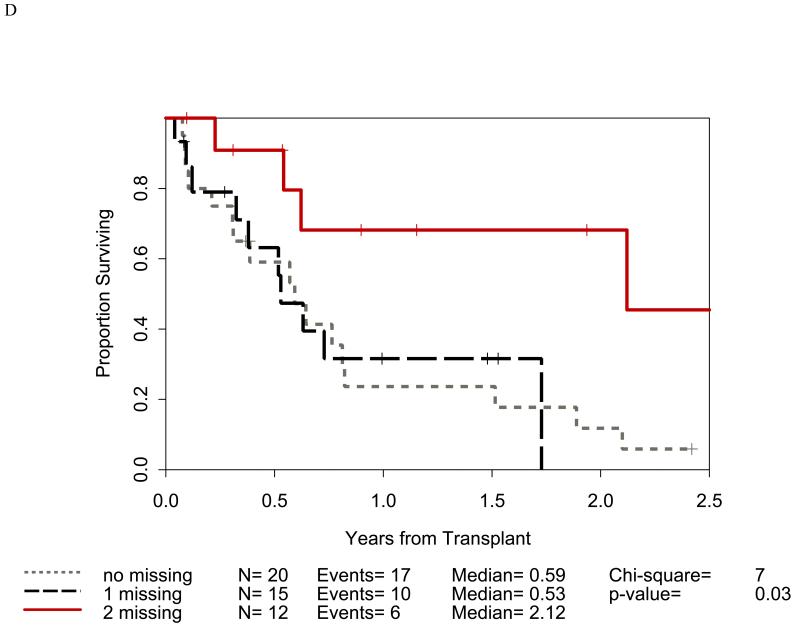
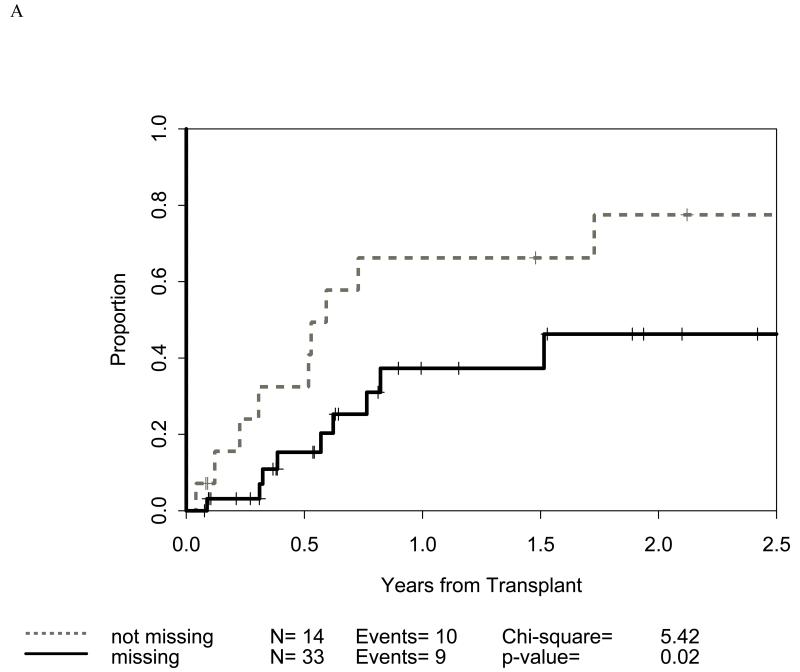
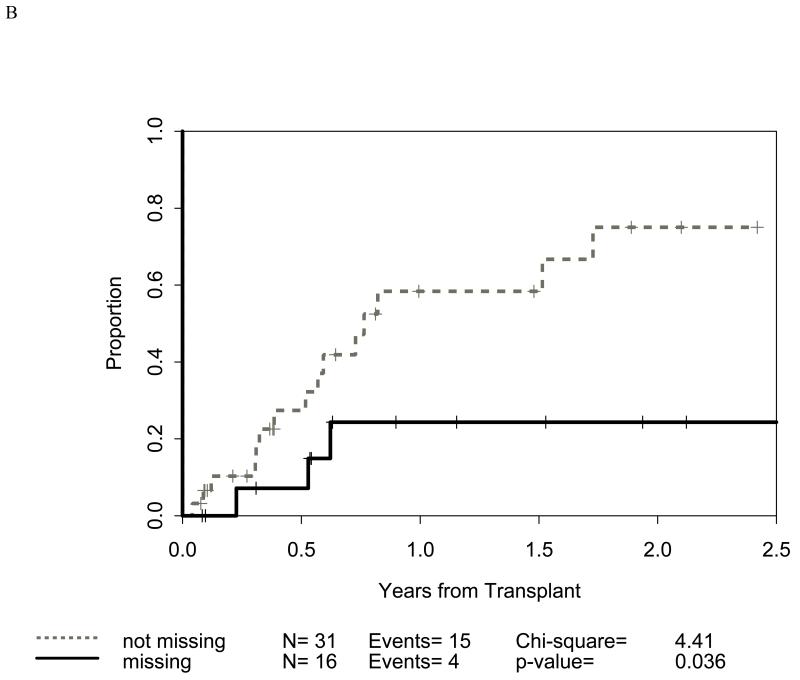
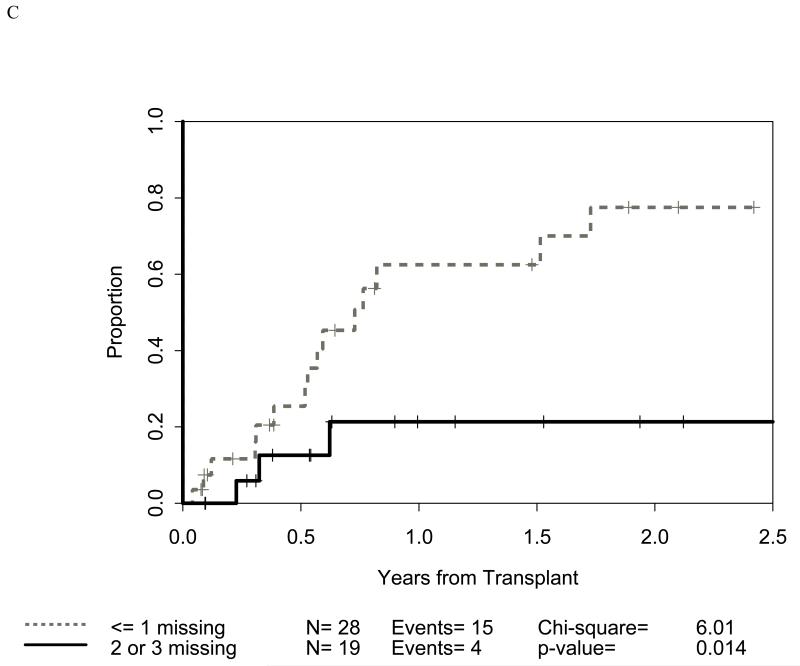
The impact of activating KIR (aKIR) and inhibitory KIR (iKIR) on OS, relapse-related mortality (RRM) and acute GVHD (aGVHD) was prospectively studied in 84 adults with high-risk hematologic malignancies receiving reduced intensity conditioning (RIC) T-cell depleted hematopoietic SCT (HSCT) from haploidentical related donors. In this clinical model, freedom from RRM is dependent on GVL effect. Patients were divided into myeloid (n=49) and lymphoid (n=35) malignancy groups. KIR-ligand and ligand-ligand models were studied in both GVH and rejection directions and statistically correlated with outcome measures. In the myeloid group, OS was higher (P=0.009) and RRM was lower (P=0.036) in patients missing HLA-C group2 ligand to donor iKIR. OS was higher if patients had >1 missing ligand (P=0.018). In lymphoid malignancy, missing ligand to donor KIR had no impact on OS or RRM. However, OS was better with donor aKIR 2DS2 (P=0.028). There was a trend towards shorter OS in recipient with KIR 2DS1, 2DS5 and 3DS1, although sample sizes were too small to provide inferential statistics. Findings in lymphoid malignancy patients should be further studied. These results suggest that the absence of appropriate HLA ligands in the recipient to donor iKIR may induce GVL without aGVHD in myeloid malignancy patients undergoing TCD-RIC transplants.
Figures
References
-
- Ruggeri L, Capanni M, Urbani E, Perruccio K, Shlomchik WD, Tosti A, et al. Effectiveness of donor natural killer cell alloreactivity in mismatched hematopoietic transplants. Science. 2002 Mar 15;295(5562):2097–100. - PubMed
-
- Hale G, Zhang MJ, Bunjes D, Prentice HG, Spence D, Horowitz MM, et al. Improving the Outcome of Bone Marrow Transplantation by Using CD52 Monoclonal Antibodies to Prevent Graft-Versus-Host Disease and Graft Rejection. Blood. 1998 Dec 15;92(12):4581–90. - PubMed
-
- Morris E, Thomson K, Craddock C, Mahendra P, Milligan D, Cook G, et al. Outcomes after alemtuzumab-containing reduced-intensity allogeneic transplantation regimen for relapsed and refractory non-Hodgkin lymphoma. Blood. 2004 Dec 15;104(13):3865–71. - PubMed
-
- Rizzieri DA, Koh LP, Long GD, Gasparetto C, Sullivan KM, Horwitz M, et al. Partially Matched, Nonmyeloablative Allogeneic Transplantation: Clinical Outcomes and Immune Reconstitution. J Clin Oncol. 2007 Feb 20;25(6):690–7. - PubMed
-
- Barrett AJ. Understanding and harnessing the graft-versus-leukaemia effect. Br J Haematol. 2008 Sep;142(6):877–88. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
