

Lamotrigine XR conversion to monotherapy: first study using a historical control group
- PMID: 22139591
- PMCID: PMC3271149
- DOI: 10.1007/s13311-011-0088-3
Lamotrigine XR conversion to monotherapy: first study using a historical control group
Abstract
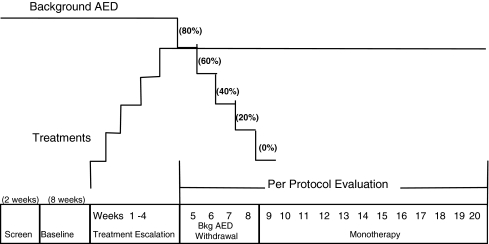
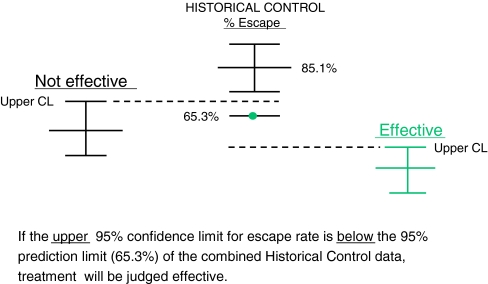
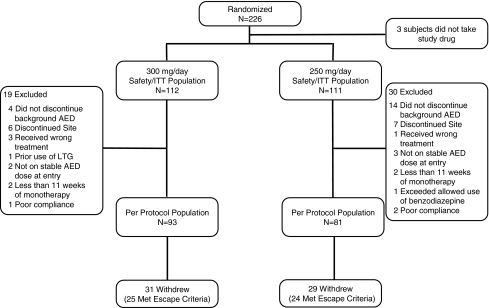
The efficacy and safety of lamotrigine extended-release tablets (LTG XR) as monotherapy for partial seizures were evaluated using the conversion-to-monotherapy design, and historical data as the control. This methodology was recently approved by the United States Food and Drug Administration, and this study is the first historical control design in epilepsy to complete enrollment. Patients ≥13 years old with uncontrolled partial epilepsy receiving monotherapy with valproate or a noninducing antiepileptic drug were converted to once-daily LTG XR (250 mg or 300 mg) as monotherapy and were followed up for 12 additional weeks. Efficacy was measured by the proportion of patients meeting predefined escape criteria for seizure worsening compared with aggregated pseudoplacebo control data from 8 previously conducted conversion-to-monotherapy trials. Nonoverlap of the 95% confidence limit for LTG XR and the 95% prediction interval of the historical control denotes efficacy. Of 226 randomized patients, 174 (93 in 300 mg/day group and 81 in 250 mg/day group) started withdrawal of the background AED and were evaluated for escape. In the historical control analysis population, the lower 95% prediction interval of the historical control (65.3%) was not overlapped by the upper 95% confidence limit of either LTG XR (300 mg/day; 37.2%) or LTG XR (250 mg/day; 43.4%). Adverse events were reported in 53% and 61% of patients receiving LTG XR (300 mg/day and 250 mg/day, respectively). LTG XR (250 mg or 300 mg once daily) is effective for conversion-to-monotherapy treatment of partial seizures in patients ≥13 years old.
Trial registration: ClinicalTrials.gov NCT00355082.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
