

Review
doi: 10.1002/lt.22467.
Cell therapies for liver diseases
Affiliations
- PMID: 22140063
- PMCID: PMC3245367
- DOI: 10.1002/lt.22467
Item in Clipboard
Review
Cell therapies for liver diseases
Liver Transpl.
2012 Jan.
Abstract
Cell therapies, which include bioartificial liver support and hepatocyte transplantation, have emerged as potential treatments for a variety of liver diseases. Acute liver failure, acute-on-chronic liver failure, and inherited metabolic liver diseases are examples of liver diseases that have been successfully treated with cell therapies at centers around the world. Cell therapies also have the potential to be widely applied to other liver diseases, including noninherited liver diseases and liver cancer, and to improve the success of liver transplantation. Here we briefly summarize current concepts of cell therapy for liver diseases.
Copyright © 2011 American Association for the Study of Liver Diseases.
Figures

A variety of cell types can be induced to form the parenchymal cells in the liver. Hepatocytes can divide to produce daughter hepatocytes; bone marrow cells can add genetic material by fusing with hepatocytes. Oval cells are resident precursor cells for cholangiocytes and hepatocytes. Stem cells can produce all cells in the liver. Fetal liver cells are an experimental source for hepatocytes and choloangiocytes. (by permission from John Wiley and Sons (98))
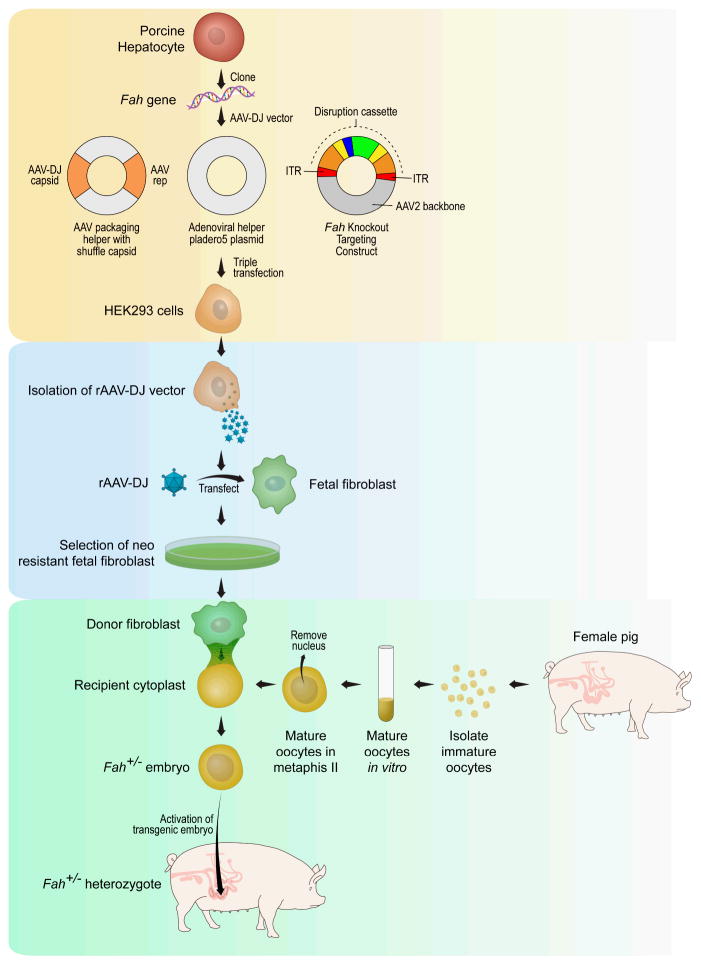
The process of cloning genetic knock-out pigs involves three steps: 1) create the targeting construct with the disruption cassette with production in HEK293 cells (shaded yellow), 2) Select for clones of porcine fetal fibroblasts that have been successfully transfected with the targeting construct (shaded light blue), 3) Produce genetically engineered piglets by somatic cell nuclear transfer – fusion of a targeted porcine fetal fibroblast with an enucleated pig embryo (shaded aqua blue).

Summary schematic of approaches to hepatocyte transplantation for treatment of inherited metabolic disease. The standard procedure under clinical evaluation uses cryopreserved human hepatocytes from donor human liver (shaded green). Alternative procedures to produce transplantable hepatocyte-like cells from human stem cells are also under development. Also under development are individualized approaches to the treatment of inherited metabolic disease by ex vivo gene therapy and in vivo cell transplantation. The individualized approach would involve production of hepatocytes from the patients own cells and thereby avoid the need for immunosuppression. Patient derived hepatocytes may be produced in vitro or expanded in vivo in genetically engineered animals such as the FAH-deficient pig. Patient derived hepatocytes could also be utilized in an extracorporeal bioartificial liver.
References
-
- Kobayashi N, Noguchi H, Fujiwara T, Westerman KA, Leboulch P, Tanaka N. Establishment of a highly differentiated immortalized adult human hepatocyte cell line by retroviral gene transfer. Transplantation proceedings. 2000;32(7):2368–9. - PubMed
-
- Han B, Lu Y, Meng B, Qu B. Cellular loss after allogenic hepatocyte transplantation. Transplantation. 2009;87:2009. - PubMed
-
- Matas AJ, Sutherland DE, Steffes MW, Mauer SM, Sowe A, Simmons RL, et al. Hepatocellular transplantation for metabolic deficiencies: decrease of plasms bilirubin in Gunn rats. Science. 1976;192(4242):892–4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical