

Need for speed: better movement quality during faster task performance after stroke
- PMID: 22140198
- PMCID: PMC3325333
- DOI: 10.1177/1545968311425926
Need for speed: better movement quality during faster task performance after stroke
Abstract
Background: . Although slow and insufficient muscle activation is a hallmark of hemiparesis poststroke, movement speed is rarely emphasized during upper-extremity rehabilitation. Moving faster may increase the intensity of task-specific training, but positive and/or negative effects on paretic-limb movement quality are unknown.
Objective: . To determine whether moving quickly instead of at a preferred speed either enhances or impairs paretic-limb task performance after stroke.
Methods: . A total of 16 people with poststroke hemiparesis and 11 healthy controls performed reach-grasp-lift movements at their preferred speed and as fast as possible, using palmar and 3-finger grip types. The authors measured durations of the reach and grasp phases, straightness of the reach path, thumb-index finger separation (aperture), efficiency of finger movement, and grip force.
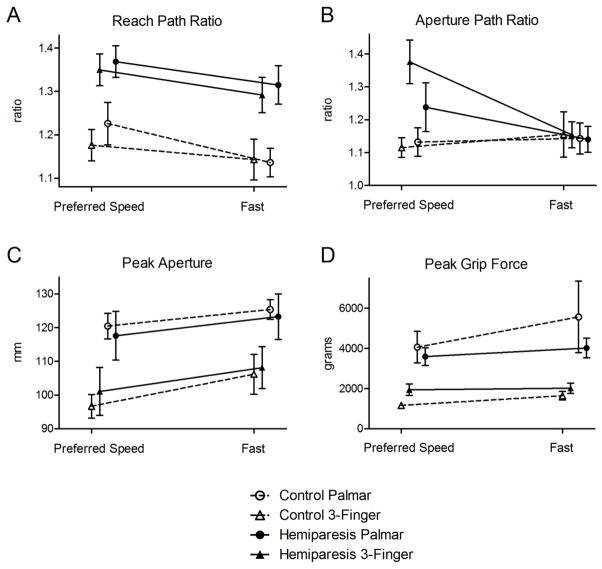
Results: . Reach and grasp phase durations decreased in the fast condition in both groups, showing that participants were able to move more quickly when asked. When moving fast, the hemiparetic group had reach durations equal to those of healthy controls moving at their preferred speed. Movement quality also improved. Reach paths were straighter, and peak apertures were greater in both groups in the fast condition. The group with hemiparesis also showed improved efficiency of finger movement. Differences in peak grip force across speed conditions did not reach significance.
Conclusions: . People with hemiparesis who can perform reach-grasp-lift movements with a 3-finger grip can move faster than they choose to, and when they do, movement quality improves. Simple instructions to move faster could be a cost-free and effective means of increasing rehabilitation intensity after stroke.
Figures




References
-
- Adkins DL, Boychuk J, Remple MS, Kleim JA. Motor training induces experience-specific patterns of plasticity across motor cortex and spinal cord. J Appl Physiol. 2006;101:1776–1782. - PubMed
-
- Mueller MJ, Maluf KS. Tissue adaptation to physical stress: A proposed “Physical stress theory” To guide physical therapist practice, education, and research. Phys Ther. 2002;82:383–403. - PubMed
-
- Askim T, Indredavik B, Vangberg T, Haberg A. Motor network changes associated with successful motor skill relearning after acute ischemic stroke: A longitudinal functional magnetic resonance imaging study. Neurorehabil Neural Repair. 2009;23:295–304. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
