

Voluntary medical male circumcision: modeling the impact and cost of expanding male circumcision for HIV prevention in eastern and southern Africa
- PMID: 22140367
- PMCID: PMC3226464
- DOI: 10.1371/journal.pmed.1001132
Voluntary medical male circumcision: modeling the impact and cost of expanding male circumcision for HIV prevention in eastern and southern Africa
Abstract
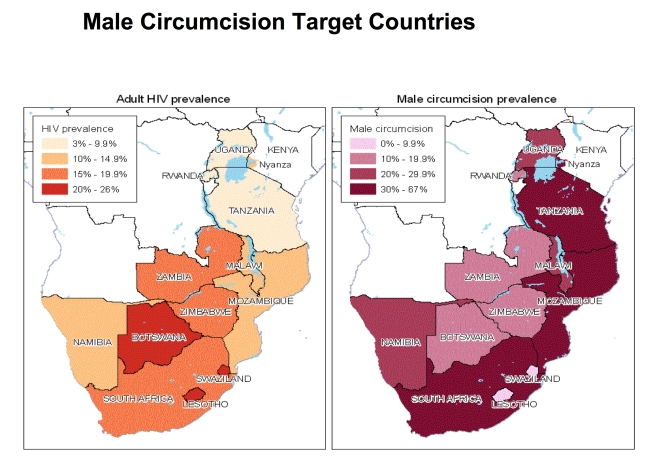
Background: There is strong evidence showing that voluntary medical male circumcision (VMMC) reduces HIV incidence in men. To inform the VMMC policies and goals of 13 priority countries in eastern and southern Africa, we estimate the impact and cost of scaling up adult VMMC using updated, country-specific data.
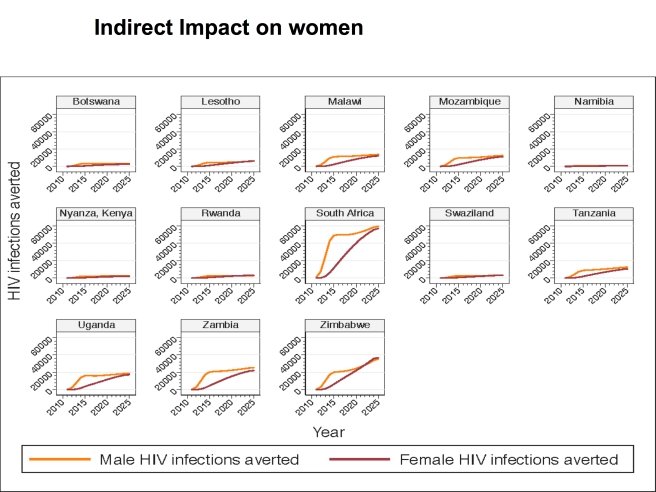
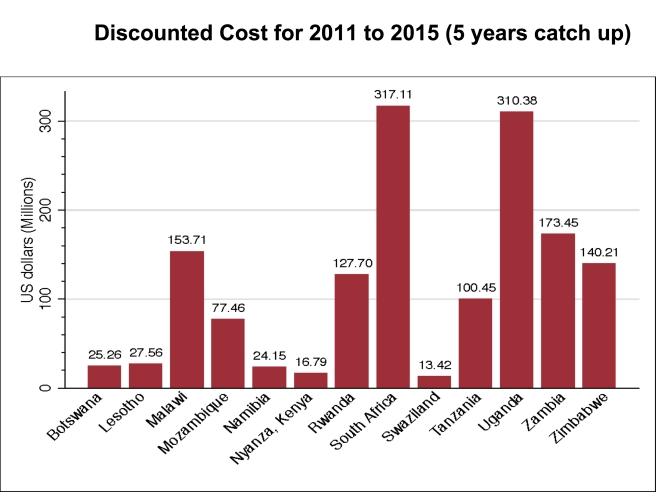
Methods and findings: We use the Decision Makers' Program Planning Tool (DMPPT) to model the impact and cost of scaling up adult VMMC in Botswana, Lesotho, Malawi, Mozambique, Namibia, Rwanda, South Africa, Swaziland, Tanzania, Uganda, Zambia, Zimbabwe, and Nyanza Province in Kenya. We use epidemiologic and demographic data from recent household surveys for each country. The cost of VMMC ranges from US$65.85 to US$95.15 per VMMC performed, based on a cost assessment of VMMC services aligned with the World Health Organization's considerations of models for optimizing volume and efficiencies. Results from the DMPPT models suggest that scaling up adult VMMC to reach 80% coverage in the 13 countries by 2015 would entail performing 20.34 million circumcisions between 2011 and 2015 and an additional 8.42 million between 2016 and 2025 (to maintain the 80% coverage). Such a scale-up would result in averting 3.36 million new HIV infections through 2025. In addition, while the model shows that this scale-up would cost a total of US$2 billion between 2011 and 2025, it would result in net savings (due to averted treatment and care costs) amounting to US$16.51 billion.
Conclusions: This study suggests that rapid scale-up of VMMC in eastern and southern Africa is warranted based on the likely impact on the region's HIV epidemics and net savings. Scaling up of safe VMMC in eastern and southern Africa will lead to a substantial reduction in HIV infections in the countries and lower health system costs through averted HIV care costs.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Auvert B, Taljaard D, Lagarde E, Sobngwi-Tambekou J, Sitta R, et al. Randomized, controlled intervention trial of male circumcision for reduction of HIV infection risk: The ANRS 1265 Trial. PLoS Med. 2005;2:e298. doi: 10.1371/journal.pmed.0020298. - DOI - PMC - PubMed
-
- Bailey RC, Moses S, Parker CB, Agot K, Maclean I, et al. Male circumcision for HIV prevention in young men in Kisumu, Kenya: A randomised controlled trial. Lancet. 2007;369:643–656. - PubMed
-
- Gray RH, Kigozi G, Serwadda D, Makumbi F, Watya S, et al. Male circumcision for HIV prevention in men in Rakai, Uganda: A randomised trial. Lancet. 2007;369:657–666. - PubMed
-
- World Health Organization, Joint United Nations Programme on HIV/AIDS. New data on male circumcision and HIV prevention: policy and programme implications. 2007. Available: http://libdoc.who.int/publications/2007/9789241595988_eng.pdf. Accessed 31 October 2011.
-
- Alsallaq R, Abu-Raddad L. Male circumcision is a leading factor behind the differential HIV prevalence in sub-Saharan Africa [poster MOPE0254]. 2008. XVII International AIDS Conference; Mexico City, Mexico; August 2008.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
