

Voluntary medical male circumcision: a framework analysis of policy and program implementation in eastern and southern Africa
- PMID: 22140368
- PMCID: PMC3226465
- DOI: 10.1371/journal.pmed.1001133
Voluntary medical male circumcision: a framework analysis of policy and program implementation in eastern and southern Africa
Abstract
Background: Following confirmation of the effectiveness of voluntary medical male circumcision (VMMC) for HIV prevention, the World Health Organization and the Joint United Nations Programme on HIV/AIDS issued recommendations in 2007. Less than 5 y later, priority countries are at different stages of program scale-up. This paper analyzes the progress towards the scale-up of VMMC programs. It analyzes the adoption of VMMC as an additional HIV prevention strategy and explores the factors may have expedited or hindered the adoption of policies and initial program implementation in priority countries to date.
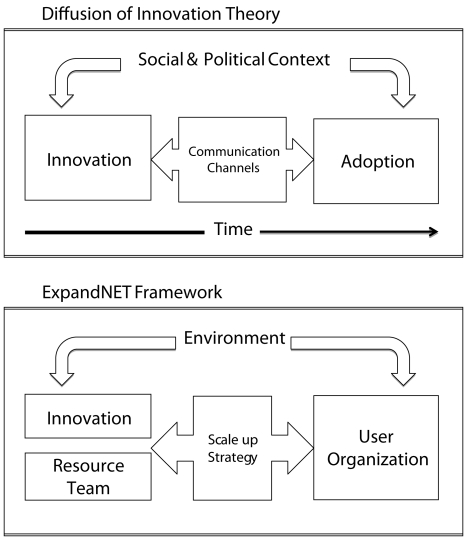
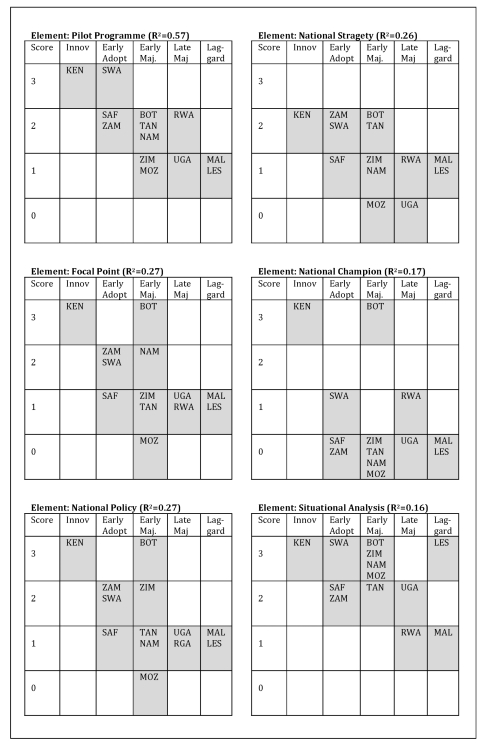
Methods and findings: VMMCs performed in priority countries between 2008 and 2010 were recorded and used to classify countries into five adopter categories according to the Diffusion of Innovations framework. The main predictors of VMMC program adoption were determined and factors influencing subsequent scale-up explored. By the end of 2010, over 550,000 VMMCs had been performed, representing approximately 3% of the target coverage level in priority countries. The "early adopter" countries developed national VMMC policies and initiated VMMC program implementation soon after the release of the WHO recommendations. However, based on modeling using the Decision Makers' Program Planning Tool (DMPPT), only Kenya appears to be on track towards achievement of the DMPPT-estimated 80% coverage goal by 2015, having already achieved 61.5% of the DMPPT target. None of the other countries appear to be on track to achieve their targets. Potential predicators of early adoption of male circumcision programs include having a VMMC focal person, establishing a national policy, having an operational strategy, and the establishment of a pilot program.
Conclusions: Early adoption of VMMC policies did not necessarily result in rapid program scale-up. A key lesson is the importance of not only being ready to adopt a new intervention but also ensuring that factors critical to supporting and accelerating scale-up are incorporated into the program. The most successful program had country ownership and sustained leadership to translate research into a national policy and program. Please see later in the article for the Editors' Summary.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures

References
-
- Joint United Nations Programme on HIV/AIDS. Geneva: Joint United Nations Programme on HIV/AIDS; 2010. Global report: UNAIDS report on global AIDS epidemic 2010.
-
- Weller S, Davis-Beaty K. Condom effectiveness in reducing heterosexual HIV transmission. Cochrane Database Syst Rev 2002. 2002. CD003255 - PubMed
-
- DeCock K, Fowler M, Mercier E, deVincenzi I, Saba J, et al. Prevention of mother-to-child HIV transmission in resource-poor countries: translating research into policy practice. JAMA. 2000;9:1175–1182. - PubMed
-
- World Health Organization. Geneva: World Health Organization; 2010. Antiretroviral drugs for treating pregnant women and preventing HIV infection in infants: recommendations for a public health approach—2010 version. - PubMed
-
- World Health Organization. Geneva: World Health Organization; 2009. WHO, UNODC, UNAIDS technical guide for countries to set targets for universal access to HIV prevention, treatment and care for injecting drug users.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
