

The Symptom Cluster of Sleep, Fatigue and Depressive Symptoms in Breast Cancer Patients: Severity of the Problem and Treatment Options
- PMID: 22140397
- PMCID: PMC3228259
- DOI: 10.1016/j.ddmod.2011.05.001
The Symptom Cluster of Sleep, Fatigue and Depressive Symptoms in Breast Cancer Patients: Severity of the Problem and Treatment Options
Abstract
Breast cancer is the most commonly diagnosed cancer in women. Insomnia is a significant problem in breast cancer patients, affecting between 20% to 70% of newly diagnosed or recently treated cancer patients. Pain, fatigue, anxiety, and depression are also common conditions in breast cancer and often co-occur with insomnia in symptom clusters, exacerbating one another, and decreasing quality of life (QOL). There have been no clinical trials of drugs for sleep in cancer. Cognitive behavioral psychotherapies on the other hand, have shown some of the most positive results in alleviating the distressing symptoms that often accompany the breast cancer experience, but even these studies have not targeted the symptom cluster. Pharmacological as well as non-pharmacological treatments need to be explored. It might be that a combined pharmacological and behavioral treatment is most efficacious. In short, substantially more research is needed to fully understand and treat the symptom cluster of insomnia, fatigue, pain, depression and anxiety in breast cancer.
Figures
References
-
- Smigal C, Jemal A, Ward E, Cokkinides V, Smith R, Howe HL, et al. Trends in breast cancer by race and ethnicity: update 2006. CA: a Cancer Journal for Clinicians. 2006;56(3):168–183. - PubMed
-
- Kissane DW, Grabsch B, Love A, Clarke DM, Bloch S, Smith GC. Psychiatric disorder in women with early stage and advanced breast cancer: a comparative analysis. Australian and New Zeland Journal of Psychiatry. 2004;38(5):320–326. - PubMed
-
- Savard J, Simard S, Blanchet J, Ivers H, Morin CM. Prevalence, clinical characteristics, and risk factors for insomnia in the context of breast cancer. Sleep. 2001;24(5):583–90. - PubMed
-
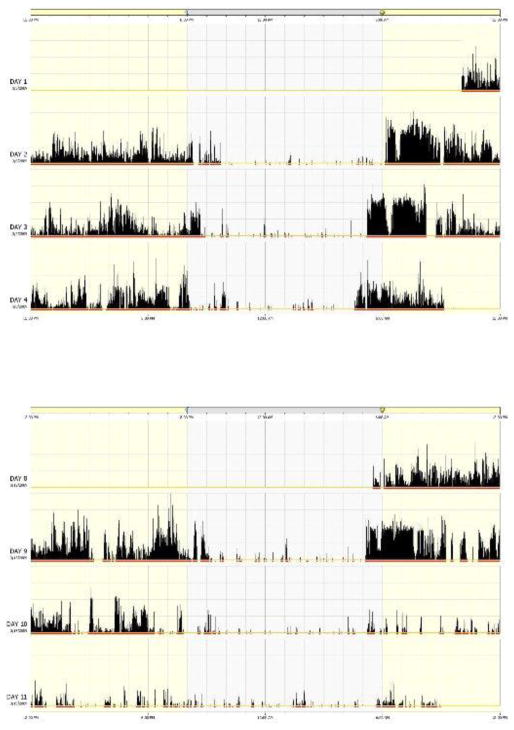
- Berger AM. Patterns of fatigue and activity and rest during adjuvant breast cancer chemotherapy. Oncol Nurs Forum. 1998;25(1):51–62. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources