

Establishing long-term efficacy in chronic disease: use of recursive partitioning and propensity score adjustment to estimate outcome in MS
- PMID: 22140424
- PMCID: PMC3227563
- DOI: 10.1371/journal.pone.0022444
Establishing long-term efficacy in chronic disease: use of recursive partitioning and propensity score adjustment to estimate outcome in MS
Abstract
Context: Establishing the long-term benefit of therapy in chronic diseases has been challenging. Long-term studies require non-randomized designs and, thus, are often confounded by biases. For example, although disease-modifying therapy in MS has a convincing benefit on several short-term outcome-measures in randomized trials, its impact on long-term function remains uncertain.
Objective: Data from the 16-year Long-Term Follow-up study of interferon-beta-1b is used to assess the relationship between drug-exposure and long-term disability in MS patients.
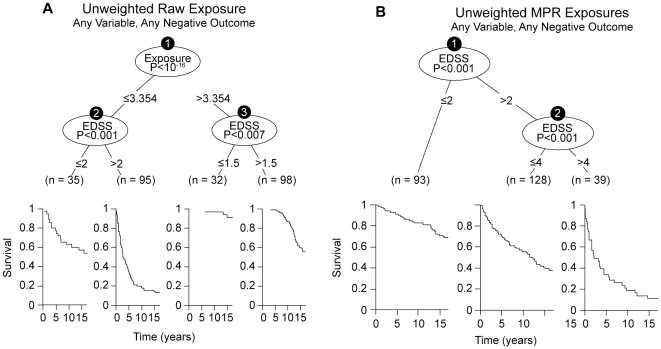
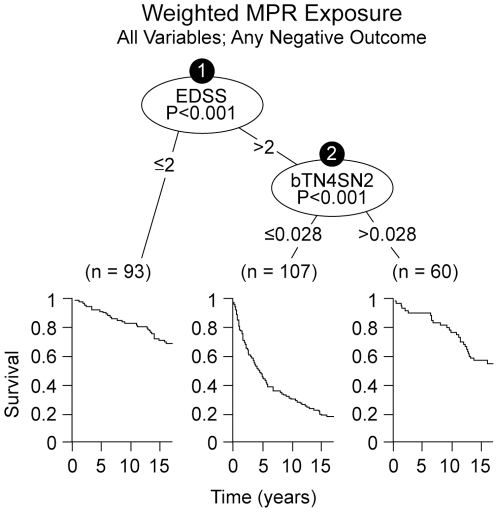
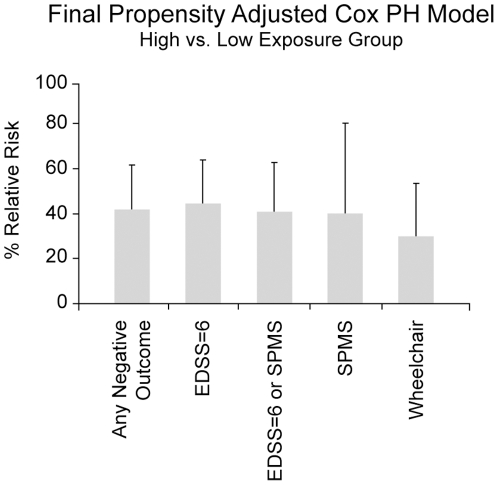
Design/setting: To mitigate the bias of outcome-dependent exposure variation in non-randomized long-term studies, drug-exposure was measured as the medication-possession-ratio, adjusted up or down according to multiple different weighting-schemes based on MS severity and MS duration at treatment initiation. A recursive-partitioning algorithm assessed whether exposure (using any weighing scheme) affected long-term outcome. The optimal cut-point that was used to define "high" or "low" exposure-groups was chosen by the algorithm. Subsequent to verification of an exposure-impact that included all predictor variables, the two groups were compared using a weighted propensity-stratified analysis in order to mitigate any treatment-selection bias that may have been present. Finally, multiple sensitivity-analyses were undertaken using different definitions of long-term outcome and different assumptions about the data.
Main outcome measure: Long-Term Disability.
Results: In these analyses, the same weighting-scheme was consistently selected by the recursive-partitioning algorithm. This scheme reduced (down-weighted) the effectiveness of drug exposure as either disease duration or disability at treatment-onset increased. Applying this scheme and using propensity-stratification to further mitigate bias, high-exposure had a consistently better clinical outcome compared to low-exposure (Cox proportional hazard ratio = 0.30-0.42; p<0.0001).
Conclusions: Early initiation and sustained use of interferon-beta-1b has a beneficial impact on long-term outcome in MS. Our analysis strategy provides a methodological framework for bias-mitigation in the analysis of non-randomized clinical data.
Trial registration: Clinicaltrials.govNCT00206635.
Conflict of interest statement
Figures
References
-
- Goodin DS, Frohman EM, Garmany GP, Halper J, Likosky WH, et al. Disease modifying therapies in multiple sclerosis: report of the Therapeutics and Technology Assessment Subcommittee of the American Academy of Neurology and the MS Council for Clinical Practice Guidelines. Neurology. 2002;58:169–178. - PubMed
-
- IFNB Multiple Sclerosis Study Group. Interferon beta-1b is effective in relapsing-remitting multiple sclerosis. I. Clinical results of a multicenter, randomized, double-blind, placebo-controlled trial. Neurology. 1993;43:655–661. - PubMed
-
- Paty DW, Li DK UBC MS/MRI Study Group, the IFNB Multiple Sclerosis Study Group. Interferon beta-1b is effective in relapsing-remitting multiple sclerosis. II. MRI analysis results of a multicenter, randomized, double-blind, placebo-controlled trial. Neurology. 1993;43:662–667. - PubMed
-
- Frohman EM, Havrdova E, Lublin F, Barkhoff F, Achiron A, et al. Most patients with multiple sclerosis or a clinically isolated demyelinating syndrome should be treated at the time of diagnosis. Arch Neurol. 2006;63:614–619. - PubMed
-
- European Study Group on interferon beta-1b in secondary progressive MS. Placebo-controlled multicentre randomised trial of interferon beta-1b in treatment of secondary progressive multiple sclerosis. Lancet. 1998;352:1491–1497. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
