

Fitness conferred by BCR-ABL kinase domain mutations determines the risk of pre-existing resistance in chronic myeloid leukemia
- PMID: 22140458
- PMCID: PMC3225363
- DOI: 10.1371/journal.pone.0027682
Fitness conferred by BCR-ABL kinase domain mutations determines the risk of pre-existing resistance in chronic myeloid leukemia
Abstract
Chronic myeloid leukemia (CML) is the first human malignancy to be successfully treated with a small molecule inhibitor, imatinib, targeting a mutant oncoprotein (BCR-ABL). Despite its successes, acquired resistance to imatinib leads to reduced drug efficacy and frequent progression of disease. Understanding the characteristics of pre-existing resistant cells is important for evaluating the benefits of first-line combination therapy with second generation inhibitors. However, due to limitations of assay sensitivity, determining the existence and characteristics of resistant cell clones at the start of therapy is difficult. Here we combined a mathematical modeling approach using branching processes with experimental data on the fitness changes (i.e., changes in net reproductive rate) conferred by BCR-ABL kinase domain mutations to investigate the likelihood, composition, and diversity of pre-existing resistance. Furthermore, we studied the impact of these factors on the response to tyrosine kinase inhibitors. Our approach predicts that in most patients, there is at most one resistant clone present at the time of diagnosis of their disease. Interestingly, patients are no more likely to harbor the most aggressive, pan-resistant T315I mutation than any other resistance mutation; however, T315I cells on average establish larger-sized clones at the time of diagnosis. We established that for patients diagnosed late, the relative benefit of combination therapy over monotherapy with imatinib is significant, while this benefit is modest for patients with a typically early diagnosis time. These findings, after pre-clinical validation, will have implications for the clinical management of CML: we recommend that patients with advanced-phase disease be treated with combination therapy with at least two tyrosine kinase inhibitors.
Conflict of interest statement
Figures
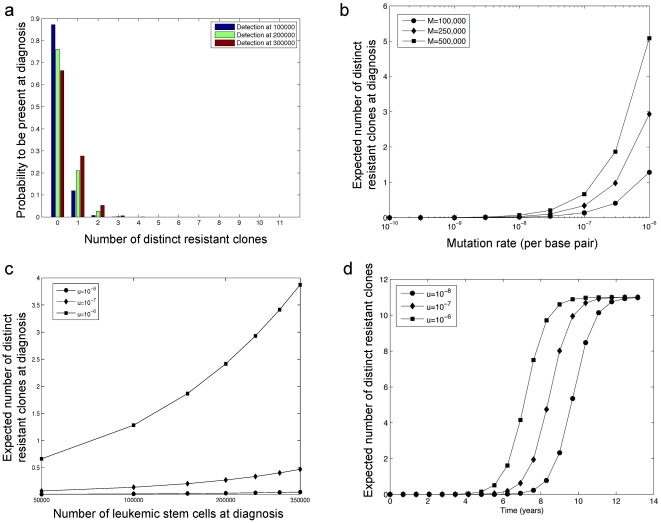
 (blue),
(blue),  (green), or
(green), or  (red) leukemic stem cells present at the time of diagnosis. The per base pair mutation rate is
(red) leukemic stem cells present at the time of diagnosis. The per base pair mutation rate is  . (b) The panel displays the expected number of resistant cell types as a function of the detection size,
. (b) The panel displays the expected number of resistant cell types as a function of the detection size,  , for varying mutation rates. (c) The expected number of resistant types at diagnosis is shown as a function of the mutation rate
, for varying mutation rates. (c) The expected number of resistant types at diagnosis is shown as a function of the mutation rate  , for varying numbers of leukemic stem cells at diagnosis,
, for varying numbers of leukemic stem cells at diagnosis,  . (d) The expected number of resistant cell types is displayed as a function of time
. (d) The expected number of resistant cell types is displayed as a function of time  in years, for varying mutation rates
in years, for varying mutation rates  .
.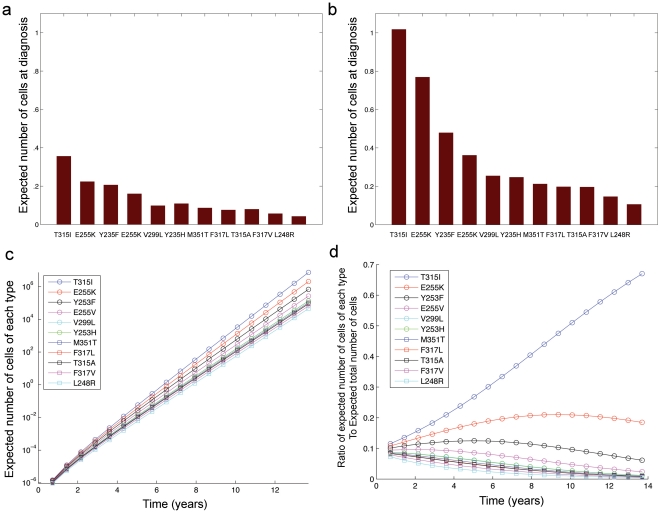
 leukemic stem cells. (b) The expected number of resistant cells of each type at diagnosis for
leukemic stem cells. (b) The expected number of resistant cells of each type at diagnosis for  leukemic stem cells is shown. (c) The panel displays the time evolution of the average number of cells of each type. (d) The ratio of the expected number of cells of each type to the expected total resistant cell number as a function of time. The mutation rate is
leukemic stem cells is shown. (c) The panel displays the time evolution of the average number of cells of each type. (d) The ratio of the expected number of cells of each type to the expected total resistant cell number as a function of time. The mutation rate is  per base per cell division for all panels.
per base per cell division for all panels.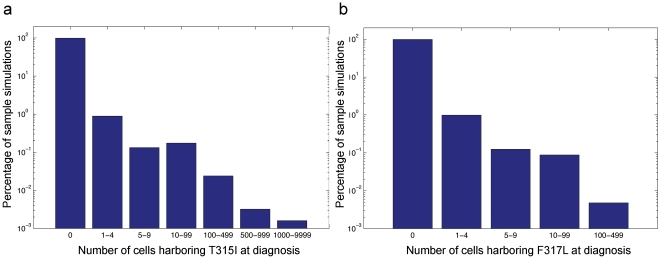
 and
and  , and simulations are run for 100,000 samples.
, and simulations are run for 100,000 samples.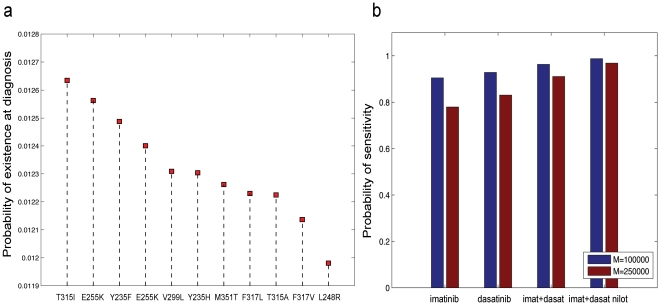
 and
and  . (b) The probability that the leukemic stem cell population is free of mutants conferring resistance to imatinib, dasatinib, imatinib plus dasatinib, and all three drugs at detection time. Parameters are
. (b) The probability that the leukemic stem cell population is free of mutants conferring resistance to imatinib, dasatinib, imatinib plus dasatinib, and all three drugs at detection time. Parameters are  (red),
(red),  (blue), and
(blue), and  .
.References
-
- Shtivelman E, Lifshitz B, Gale R, Canaani E. Fused transcript of abl and bcr genes in chronic myelogenous leukaemia. Nature. 1985;315:550–554. - PubMed
-
- Nowell P. Phytohemagglutnin: An initiator of mitosis in cultures of normal human leukocytes. Cancer Research. 1960;20:462–466. - PubMed
-
- Goldman J, Melo J. Chronic myeloid leukemia advances in biology and new approaches to treatment. New England Journal of Medicine. 2003;349:1451–1464. - PubMed
-
- Druker BJ, Talpaz M, Resta D, Peng B, Buchdunger E, et al. Efficacy and safety of a specific inhibitor of the BCR-ABL tyrosine kinase in chronic myeloid leukemia. New England Journal of Medicine. 2001;344:1031–1037. - PubMed
-
- Hochhaus A. Chronic myelogenous leukemia (CML): resistance to tyrosine kinase inhibitors. Annals of Oncology. 2006;17:274–279. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
