

Visceral leishmaniasis in the Indian subcontinent: modelling epidemiology and control
- PMID: 22140589
- PMCID: PMC3226461
- DOI: 10.1371/journal.pntd.0001405
Visceral leishmaniasis in the Indian subcontinent: modelling epidemiology and control
Abstract
Background: In the Indian subcontinent, about 200 million people are at risk of developing visceral leishmaniasis (VL). In 2005, the governments of India, Nepal and Bangladesh started the first regional VL elimination program with the aim to reduce the annual incidence to less than 1 per 10,000 by 2015. A mathematical model was developed to support this elimination program with basic quantifications of transmission, disease and intervention parameters. This model was used to predict the effects of different intervention strategies.
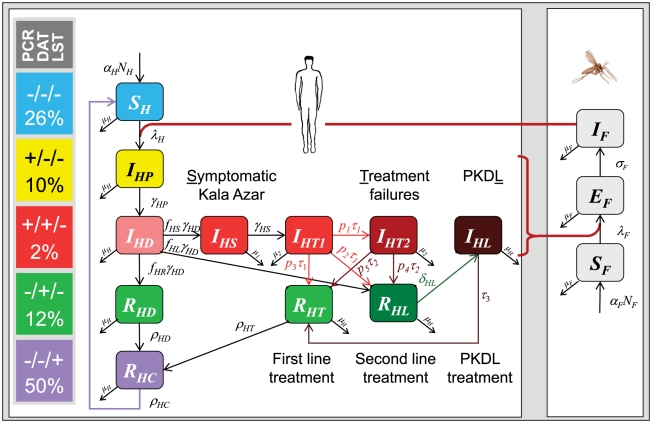
Methods and findings: Parameters on the natural history of Leishmania infection were estimated based on a literature review and expert opinion or drawn from a community intervention trial (the KALANET project). The transmission dynamic of Leishmania donovani is rather slow, mainly due to its long incubation period and the potentially long persistence of parasites in infected humans. Cellular immunity as measured by the Leishmanin skin test (LST) lasts on average for roughly one year, and re-infection occurs in intervals of about two years, with variation not specified. The model suggests that transmission of L. donovani is predominantly maintained by asymptomatically infected hosts. Only patients with symptomatic disease were eligible for treatment; thus, in contrast to vector control, the treatment of cases had almost no effect on the overall intensity of transmission.
Conclusions: Treatment of Kala-azar is necessary on the level of the individual patient but may have little effect on transmission of parasites. In contrast, vector control or exposure prophylaxis has the potential to efficiently reduce transmission of parasites. Based on these findings, control of VL should pay more attention to vector-related interventions. Cases of PKDL may appear after years and may initiate a new outbreak of disease; interventions should therefore be long enough, combined with an active case detection and include effective treatment.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Boelaert M, Meheus F, Sanchez A, Singh SP, Vanlerberghe V, et al. The poorest of the poor: a poverty appraisal of households affected by visceral leishmaniasis in Bihar, India. Trop Med Int Health. 2009;14:639–644. - PubMed
-
- Chappuis F, Sundar S, Hailu A, Ghalib H, Rijal S, et al. Visceral leishmaniasis: what are the needs for diagnosis, treatment and control? Nat Rev Microbiol. 2007;5:873–882. - PubMed
-
- Ashford RW. The leishmaniases as emerging and reemerging zoonoses. Int J Parasitol. 2000;30:1269–1281. - PubMed
-
- Desjeux P. Leishmaniasis: current situation and new perspectives. Comp Immunol Microbiol Infect Dis. 2004;27:305–318. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
