

Identifying a high stroke risk subgroup in individuals with heart failure
- PMID: 22142776
- PMCID: PMC3326204
- DOI: 10.1016/j.jstrokecerebrovasdis.2011.10.012
Identifying a high stroke risk subgroup in individuals with heart failure
Abstract
Background: Heart failure (HF) is associated with an overall stroke rate that is too low to justify anticoagulation in all patients. This study was conducted to determine if vascular risk factors can identify a subgroup of individuals with heart failure with a stroke rate high enough to warrant anticoagulation.
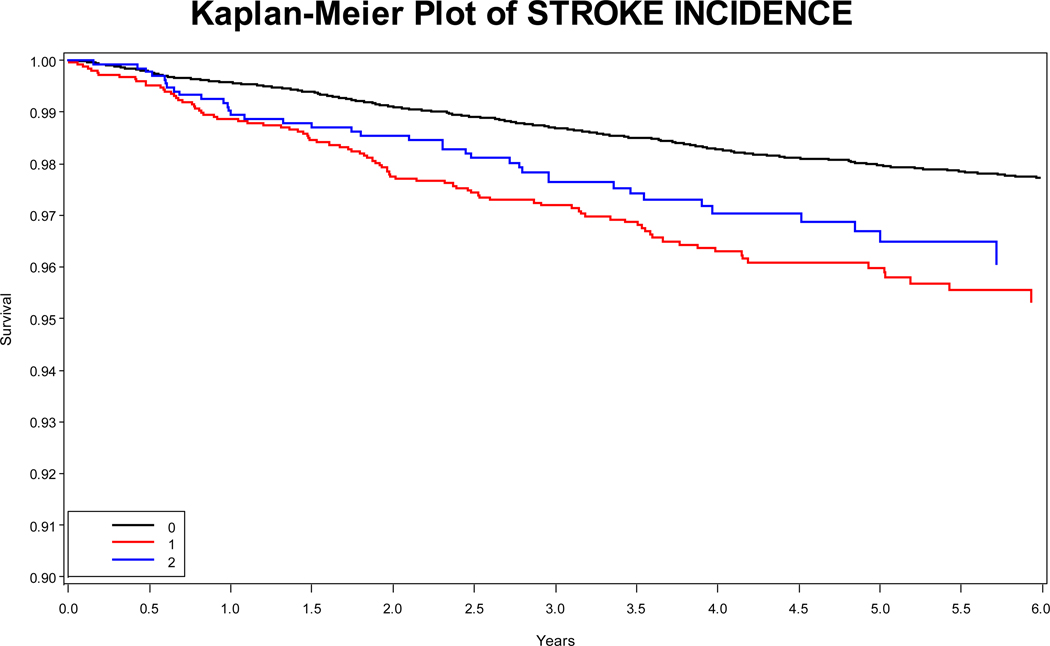
Methods: The REGARDS study is a population-based cohort of US adults aged ≥45 years. Participants are contacted every 6 months by telephone for self- or proxy-reported stroke and medical records are retrieved and adjudicated by physicians. Participants were characterized into 3 groups: HF without atrial fibrillation (AF), AF with or without HF, and neither HF nor AF. Cardiovascular risk factors at baseline were compared between participants with and without incident stroke in HF and AF. Stroke incidence was assessed in risk factor subgroups in HF participants.
Results: Of the 30,239 participants, those with missing/anomalous data were excluded. Of the remaining 28,832, 1360 (5%) had HF without AF, 2528 (9%) had AF, and 24,944 (86%) had neither. Previous stroke/transient ischemic attack (TIA; P = .0004), diabetes mellitus (DM; P = .03), and higher systolic blood pressure (P = .046) were associated with increased stroke risk in participants with HF without AF. In participants with HF without AF, stroke incidence was highest in those with previous stroke/TIA and DM (2.4 [1.1, 4.0] per 100 person-years).
Conclusions: The combination of previous stroke/TIA and DM increases the incidence of stroke in participants with HF without AF. No analyzed subgroup had a stroke rate high enough to make it likely that the benefits of warfarin would outweigh the risks.
Copyright © 2013 National Stroke Association. Published by Elsevier Inc. All rights reserved.
Figures
Similar articles
-
The increased risk of stroke/transient ischemic attack in women with a cardiac implantable electronic device is not associated with a higher atrial fibrillation burden.Europace. 2017 Nov 1;19(11):1767-1775. doi: 10.1093/europace/euw333. Europace. 2017. PMID: 28031277
-
Incidence of ischemic stroke or transient ischemic attack in patients with multiple risk factors with or without atrial fibrillation: a retrospective cohort study.Curr Med Res Opin. 2015;31(7):1257-66. doi: 10.1185/03007995.2015.1041469. Epub 2015 May 6. Curr Med Res Opin. 2015. PMID: 25877807
-
Incidence and predictors of ischemic stroke during hospitalization for congestive heart failure.Heart Vessels. 2016 Jul;31(7):1154-61. doi: 10.1007/s00380-015-0719-4. Epub 2015 Jul 29. Heart Vessels. 2016. PMID: 26219729
-
Advancing Research on the Complex Interrelations Between Atrial Fibrillation and Heart Failure: A Report From a US National Heart, Lung, and Blood Institute Virtual Workshop.Circulation. 2020 Jun 9;141(23):1915-1926. doi: 10.1161/CIRCULATIONAHA.119.045204. Epub 2020 Jun 8. Circulation. 2020. PMID: 32511001 Free PMC article. Review.
-
Identification and Mapping Real-World Data Sources for Heart Failure, Acute Coronary Syndrome, and Atrial Fibrillation.Cardiology. 2022;147(1):98-106. doi: 10.1159/000520674. Epub 2021 Nov 15. Cardiology. 2022. PMID: 34781301 Free PMC article.
Cited by
-
Risk of stroke in chronic heart failure patients with preserved ejection fraction, but without atrial fibrillation: analysis of the CHARM-Preserved and I-Preserve trials.Eur Heart J. 2017 Mar 7;38(10):742-750. doi: 10.1093/eurheartj/ehw509. Eur Heart J. 2017. PMID: 28426886 Free PMC article. Clinical Trial.
-
The impact of the lactate-to-albumin ratio on long-term mortality risk in patients with severe heart failure and type 2 diabetes.BMC Cardiovasc Disord. 2025 Mar 29;25(1):234. doi: 10.1186/s12872-025-04612-z. BMC Cardiovasc Disord. 2025. PMID: 40158175 Free PMC article.
-
Risk of stroke and bleeding in patients with heart failure and chronic kidney disease: a nationwide cohort study.ESC Heart Fail. 2018 Apr;5(2):319-326. doi: 10.1002/ehf2.12256. Epub 2018 Jan 31. ESC Heart Fail. 2018. PMID: 29383860 Free PMC article.
-
Vascular Disease and Risk Stratification for Ischemic Stroke and All-Cause Death in Heart Failure Patients without Diagnosed Atrial Fibrillation: A Nationwide Cohort Study.PLoS One. 2016 Mar 25;11(3):e0152269. doi: 10.1371/journal.pone.0152269. eCollection 2016. PLoS One. 2016. PMID: 27015524 Free PMC article.
-
Using mHealth Tools to Improve Rural Diabetes Care Guided by the Chronic Care Model.Online J Rural Nurs Health Care. 2014;14(1):43-65. doi: 10.14574/ojrnhc.v14i1.276. Online J Rural Nurs Health Care. 2014. PMID: 26029005 Free PMC article.
References
-
- Pullicino P, Homma S, Thompson JL, et al. Oral anticoagulation in patients with cardiomyopathy or heart failure in sinus rhythm. Cerebrovasc Dis. 2008;26:322–327. - PubMed
-
- Han SW, Nam HS, Kim SH, Lee, et al. Frequency and significance of cardiac sources of embolism in the TOAST classification. Cerebrovasc Dis. 2007;24:463–468. - PubMed
-
- Go AS, Hylek EM, Phillips KA, et al. Prevalence of diagnosed atrial fibrillation in adults: the AnTicoagulation and Risk Factors in Atrial Fibrillation (ATRIA) Study. JAMA. 2001 May 9;285:2370–2375. - PubMed
-
- Kannel WB, Wolf PA, Verter J. Manifestations of coronary disease predisposing to stroke. The Framingham study. JAMA. 1983;250:2942–2946. - PubMed
-
- Witt BJ, Brown RD, Jr, Jacobsen SJ, et al. Ischemic stroke after heart failure: a community-based study. Am Heart J. 2006;152:102–109. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
