

Dysautonomia: perioperative implications
- PMID: 22143168
- PMCID: PMC3296831
- DOI: 10.1097/ALN.0b013e31823db712
Dysautonomia: perioperative implications
Abstract
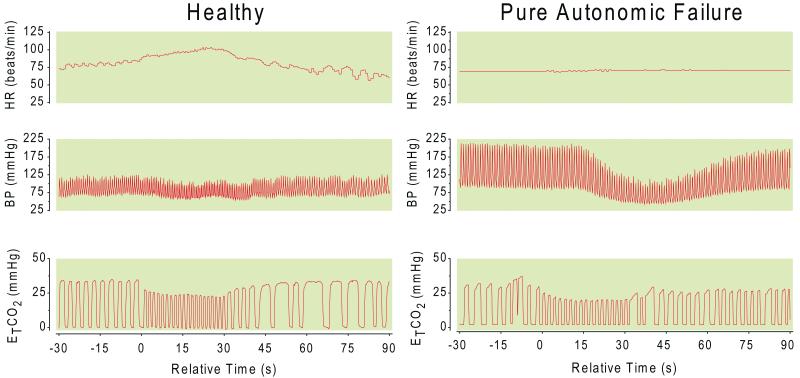
Severe autonomic failure occurs in approximately 1 in 1,000 people. Such patients are remarkable for the striking and sometimes paradoxic responses they manifest to a variety of physiologic and pharmacologic stimuli. Orthostatic hypotension is often the finding most commonly noted by physicians, but a myriad of additional and less understood findings also occur. These findings include supine hypertension, altered drug sensitivity, hyperresponsiveness of blood pressure to hypo/hyperventilation, sleep apnea, and other neurologic disturbances. In this article the authors will review the clinical pathophysiology that underlies autonomic failure, with a particular emphasis on those aspects most relevant to the care of such patients in the perioperative setting. Strategies used by clinicians in diagnosis and treatment of these patients, and the effect of these interventions on the preoperative, intraoperative, and postoperative care that these patients undergo is a crucial element in the optimized management of care in these patients.
Figures
Similar articles
-
Perioperative implications of the patient with autonomic dysfunction.Curr Opin Anaesthesiol. 2014 Jun;27(3):365-70. doi: 10.1097/ACO.0000000000000072. Curr Opin Anaesthesiol. 2014. PMID: 24722004 Review.
-
Dysautonomia: A Forgotten Condition - Part 1.Arq Bras Cardiol. 2021 Apr;116(4):814-835. doi: 10.36660/abc.20200420. Arq Bras Cardiol. 2021. PMID: 33886735 Free PMC article. English, Portuguese.
-
Syndrome of Supine Hypertension with Orthostatic Hypotension: Pathophysiology and Clinical Approach.Curr Cardiol Rev. 2020;16(1):48-54. doi: 10.2174/1573403X15666190617095032. Curr Cardiol Rev. 2020. PMID: 31215392 Free PMC article. Review.
-
Attenuated cardiac autonomic function in patients with long-COVID with impaired orthostatic hemodynamics.Clin Auton Res. 2025 Apr;35(2):301-314. doi: 10.1007/s10286-025-01107-x. Epub 2025 Jan 22. Clin Auton Res. 2025. PMID: 39841332
-
Reverse blood pressure dipping as marker of dysautonomia in Parkinson disease.Parkinsonism Relat Disord. 2018 Nov;56:82-87. doi: 10.1016/j.parkreldis.2018.06.032. Epub 2018 Jun 28. Parkinsonism Relat Disord. 2018. PMID: 30057156
Cited by
-
Anesthetic Considerations for Cataract Surgery in Patients with Parkinson's Disease: A Narrative Review.Anesth Pain Med. 2023 May 6;13(3):e136093. doi: 10.5812/aapm-136093. eCollection 2023 Jun. Anesth Pain Med. 2023. PMID: 38021330 Free PMC article. Review.
-
ANSiscope™: Can it be the crystal ball of cardiac anesthesia?Ann Card Anaesth. 2019 Jan-Mar;22(1):101-106. doi: 10.4103/aca.ACA_9_18. Ann Card Anaesth. 2019. PMID: 30648692 Free PMC article.
-
Jaw-in-a-Riley-Day: Mandibular Free Flap Reconstruction With Virtual Surgical Planning in a Patient With Familial Dysautonomia.Cureus. 2022 Jun 26;14(6):e26336. doi: 10.7759/cureus.26336. eCollection 2022 Jun. Cureus. 2022. PMID: 35911292 Free PMC article.
-
Anaesthesia for Caesarean Section in a Patient With Familial Amyloid Polyneuropathy Type I.Cureus. 2024 Dec 3;16(12):e75033. doi: 10.7759/cureus.75033. eCollection 2024 Dec. Cureus. 2024. PMID: 39634207 Free PMC article.
-
Anesthetic experience of frontotemporal dementia patient with severe autonomic dysfunction: a case report.Korean J Anesthesiol. 2017 Jun;70(3):356-360. doi: 10.4097/kjae.2017.70.3.356. Epub 2017 Feb 3. Korean J Anesthesiol. 2017. PMID: 28580089 Free PMC article.
References
-
- Shibao C, Grijalva CG, Raj SR, Biaggioni I, Griffin MR. Orthostatic hypotension-related hospitalizations in the United States. Am.J.Med. 2007;120:975–80. - PubMed
-
- Goldstein DS, Holmes C, Frank SM, Dendi R, Cannon RO, III, Sharabi Y, Esler MD, Eisenhofer G. Cardiac sympathetic dysautonomia in chronic orthostatic intolerance syndromes. Circulation. 2002;106:2358–65. - PubMed
-
- Robertson D, Hollister AS, Biaggioni I, Netterville JL, Mosqueda-Garcia R, Robertson RM. The diagnosis and treatment of baroreflex failure. N.Engl.J.Med. 1993;329:1449–55. - PubMed
-
- Robertson D. The pathophysiology and diagnosis of orthostatic hypotension. Clin.Auton.Res. 2008;18(Suppl 1):2–7. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
