

Enrolment in primary care networks: impact on outcomes and processes of care for patients with diabetes
- PMID: 22143232
- PMCID: PMC3273535
- DOI: 10.1503/cmaj.110755
Enrolment in primary care networks: impact on outcomes and processes of care for patients with diabetes
Abstract
Background: Primary care networks are a newer model of primary care that focuses on improved access to care and the use of multidisciplinary teams for patients with chronic disease. We sought to determine the association between enrolment in primary care networks and the care and outcomes of patients with diabetes.
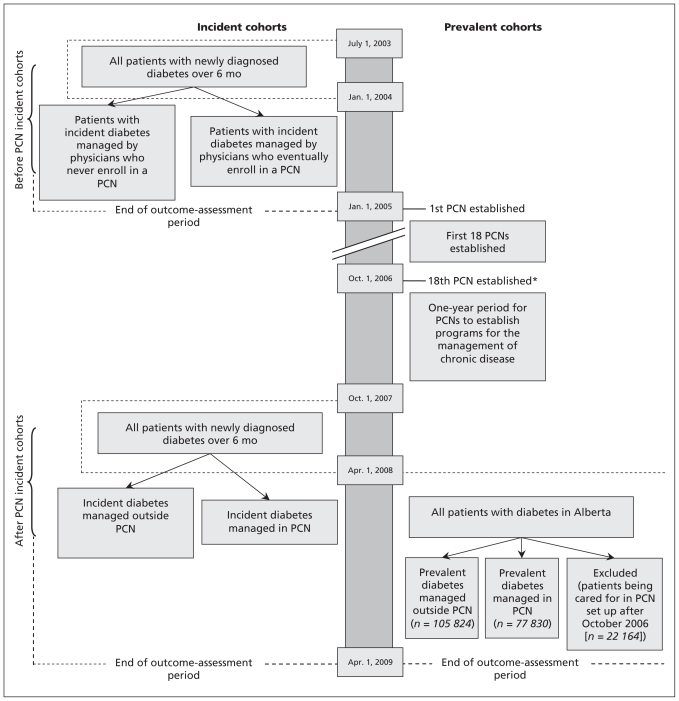
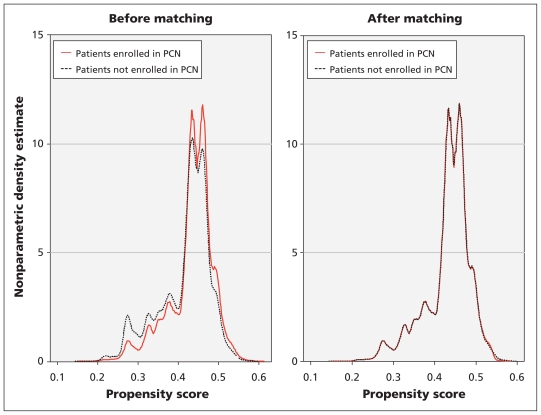
Methods: We used administrative health care data to study the care and outcomes of patients with incident and prevalent diabetes separately. For patients with prevalent diabetes, we compared those whose care was managed by physicians who were or were not in a primary care network using propensity score matching. For patients with incident diabetes, we studied a cohort before and after primary care networks were established. Each cohort was further divided based on whether or not patients were cared for by physicians enrolled in a network. Our primary outcome was admissions to hospital or visits to emergency departments for ambulatory care sensitive conditions specific to diabetes.
Results: Compared with patients whose prevalent diabetes is managed outside of primary care networks, patients in primary care networks had a lower rate of diabetes-specific ambulatory care sensitive conditions (adjusted incidence rate ratio 0.81, 95% confidence interval [CI] 0.75 to 0.87), were more likely to see an ophthalmologist or optometrist (risk ratio 1.19, 95% CI 1.17 to 1.21) and had better glycemic control (adjusted mean difference -0.067, 95% CI -0.081 to -0.052).
Interpretation: Patients whose diabetes was managed in primary care networks received better care and had better clinical outcomes than patients whose condition was not managed in a network, although the differences were very small.
Figures
References
-
- Johnson JA. Alberta diabetes atlas. Edmonton (AB): Institute of Health Economics; 2009
-
- Tonelli M, Bohm C, Pandeya S, et al. Cardiac risk factors and the use of cardioprotective medications in patients with chronic renal insufficiency. Am J Kidney Dis 2001;37:484–9 - PubMed
-
- Tonelli M, Gill J, Pandeya S, et al. Barriers to blood pressure control and angiotensin enzyme inhibitor use in Canadian patients with chronic renal insufficiency. Nephrol Dial Transplant 2002;17:1426–33 - PubMed
-
- Gaede P, Vedel P, Larsen N, et al. Multifactorial interventions and cardiovascular disease in patients with type 2 diabetes. N Engl J Med 2003;348:383–93 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical