

Surveillance of pancreatic cancer patients after surgical resection
- PMID: 22143577
- PMCID: PMC3360943
- DOI: 10.1245/s10434-011-2152-y
Surveillance of pancreatic cancer patients after surgical resection
Abstract
Background: There are no clear recommendations to guide posttreatment surveillance in patients with pancreatic cancer. Our goal was to describe the posttreatment surveillance patterns in patients undergoing curative-intent resection for pancreatic cancer.
Methods: We used Surveillance, Epidemiology, and End Results (SEER)-Medicare linked data (1992-2005) to identify CT scans and physician visits in patients with pancreatic cancer who underwent curative resection (n = 2393). Surveillance began 90 days after surgery, and patients were followed for 2 years at 6-month intervals. Patients were censored if they died, experienced recurrence of disease, or entered hospice.
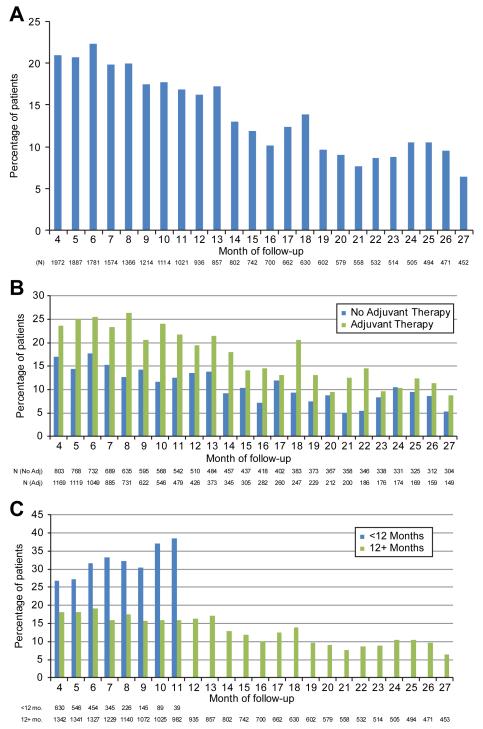
Results: A total of 2045 patients survived uncensored to the beginning of the surveillance period. CT scan use decreased from 20.9% of patients in month 4 to 6.4% in month 27. There was no temporal pattern in CT use to suggest regular surveillance. Twenty-three percent of patients did not receive a CT scan in the year after surgery, increasing to 42% the second year. Patients who underwent adjuvant therapy and patients diagnosed in later years had higher CT scan use over the surveillance periods. Most patients visited both a primary care physician and a cancer specialist in each 6-month surveillance period. Patients who visited cancer specialists were more likely to have any CT scan and to be scanned more frequently.
Conclusions: Current surveillance patterns after resection for pancreatic cancer reflect the lack of established guidelines, implying a need for evaluation and standardization of surveillance protocols. The lack of a temporal pattern in CT testing suggests that most were obtained to evaluate symptoms rather than for routine surveillance.
Figures
References
-
- Jemal A, Siegel R, Xu J, Ward E. Cancer statistics, 2010. CA Cancer J Clin. 2010 Sep-Oct;60(5):277–300. - PubMed
-
- Wagner M, Redaelli C, Lietz M, Seiler CA, Friess H, Buchler MW. Curative resection is the single most important factor determining outcome in patients with pancreatic adenocarcinoma. Br J Surg. 2004 May;91(5):586–594. - PubMed
-
- Hernandez JM, Morton CA, Al-Saadi S, et al. The natural history of resected pancreatic cancer without adjuvant chemotherapy. Am Surg. 2010 May;76(5):480–485. - PubMed
-
- Asiyanbola B, Gleisner A, Herman JM, et al. Determining pattern of recurrence following pancreaticoduodenectomy and adjuvant 5-flurouracil-based chemoradiation therapy: effect of number of metastatic lymph nodes and lymph node ratio. J Gastrointest Surg. 2009 Apr;13(4):752–759. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
