

MRI identifies plantar plate pathology in the forefoot of patients with rheumatoid arthritis
- PMID: 22143913
- PMCID: PMC3314823
- DOI: 10.1007/s10067-011-1899-7
MRI identifies plantar plate pathology in the forefoot of patients with rheumatoid arthritis
Abstract
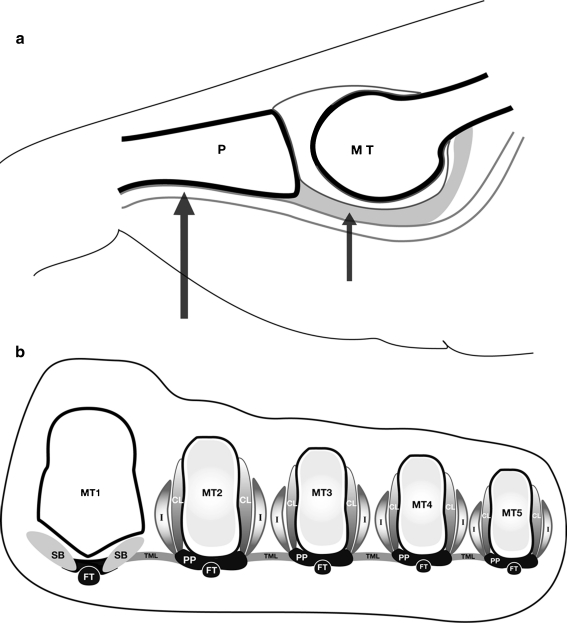
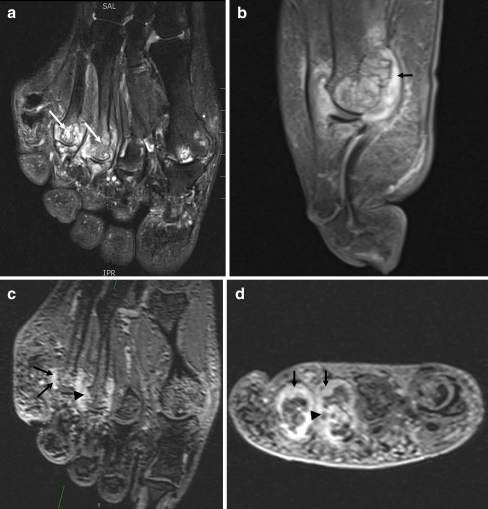
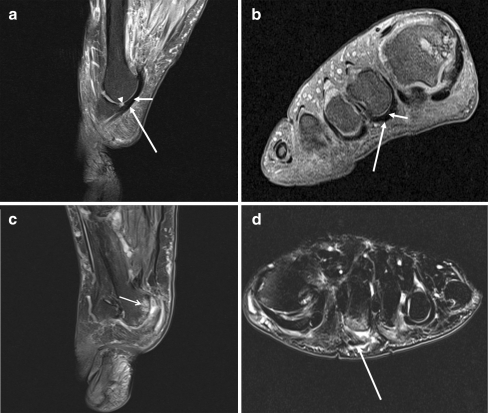
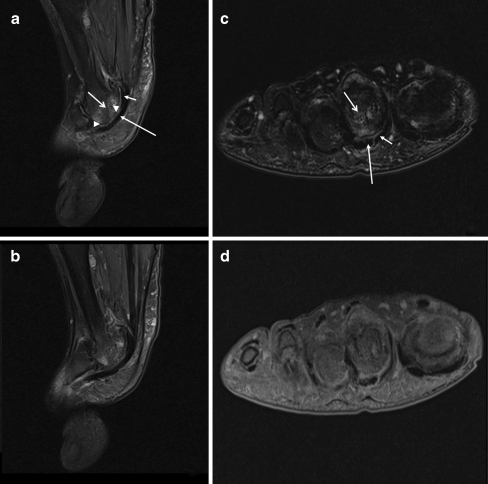
Previous cadaveric studies have suggested that forefoot deformities at the metatarsophalangeal (MTP) joints in patients with rheumatoid arthritis (RA) might result from the failure of the ligamentous system and displacement of the plantar plates. This study aimed to examine the relationship between plantar plate pathology and the rheumatoid arthritis magnetic resonance imaging score (RAMRIS) of the lesser (second to fifth) MTP joints in patients with RA using high-resolution 3 T magnetic resonance imaging (MRI). In 24 patients with RA, the forefoot was imaged using 3 T MRI. Proton density fat-suppressed, T2-weighted fat-suppressed and T1-weighted post gadolinium sequences were acquired through 96 lesser MTP joints. Images were scored for synovitis, bone marrow oedema and bone erosion using the RAMRIS system and the plantar plates were assessed for pathology. Seventeen females and 7 males with a mean age of 55.5 years (range 37-71) and disease duration of 10.6 years (range 0.6-36) took part in the study. Plantar plate pathology was most frequently demonstrated on MRI at the fifth MTP joint. An association was demonstrated between plantar plate pathology and RAMRIS-reported synovitis, bone marrow oedema and bone erosion at the fourth and fifth MTP joints. In patients with RA, 3 T MRI demonstrates that plantar plate pathology at the lesser MTP joints is associated with features of disease severity. Plantar plate pathology is more common at the fourth and fifth MTP joints in subjects with RA in contrast to the predilection for the second MTP reported previously in subjects without RA.
Figures
References
-
- Johnston RB, 3rd, Smith J, Daniels T, Johnston RB, 3rd, Smith J, Daniels T. The plantar plate of the lesser toes: an anatomical study in human cadavers. Foot Ankle Int. 1994;15(5):276–282. - PubMed
-
- Yao L, Do HM, Cracchiolo A, Farahani K, Yao L, Do HM, Cracchiolo A, Farahani K. Plantar plate of the foot: findings on conventional arthrography and MR imaging. AJR Am J Roentgenol. 1994;163(3):641–644. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
