

QCT measures of bone strength at the thoracic and lumbar spine: the Framingham Study
- PMID: 22143959
- PMCID: PMC3728822
- DOI: 10.1002/jbmr.1482
QCT measures of bone strength at the thoracic and lumbar spine: the Framingham Study
Abstract
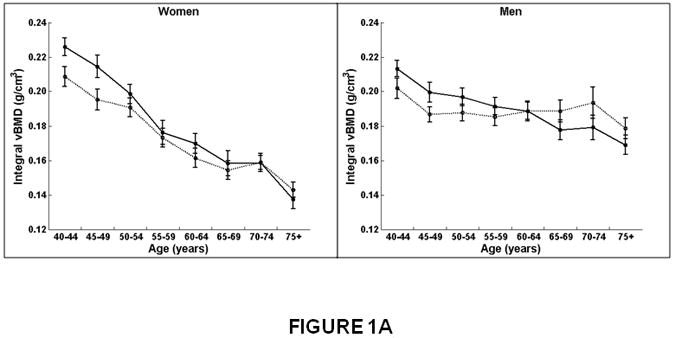
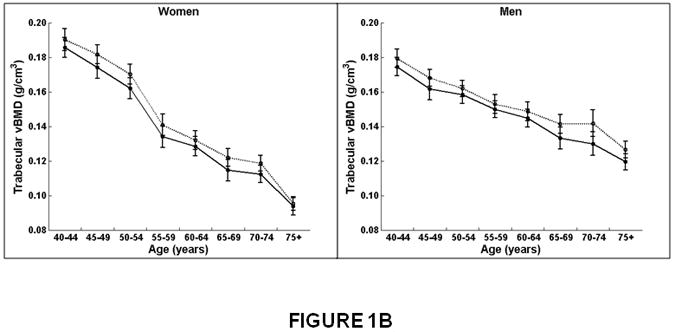
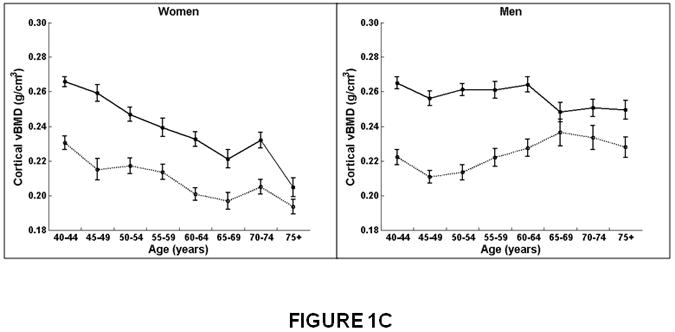
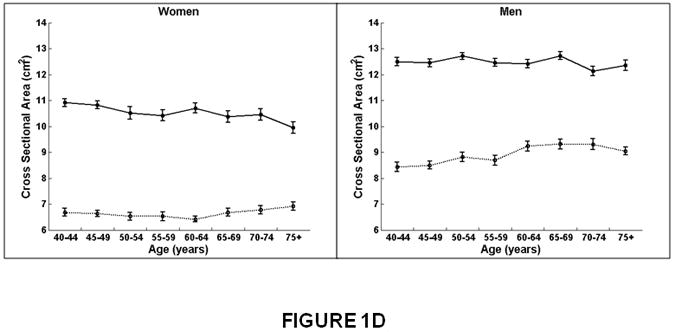
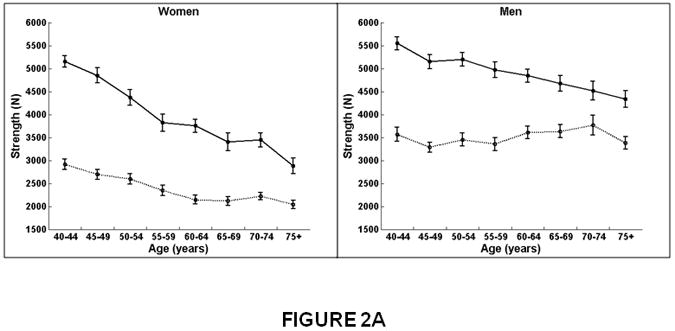
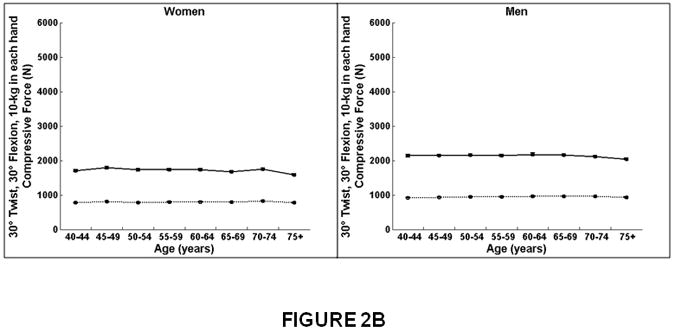
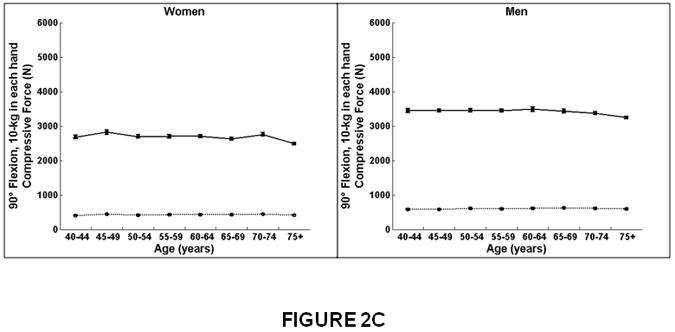
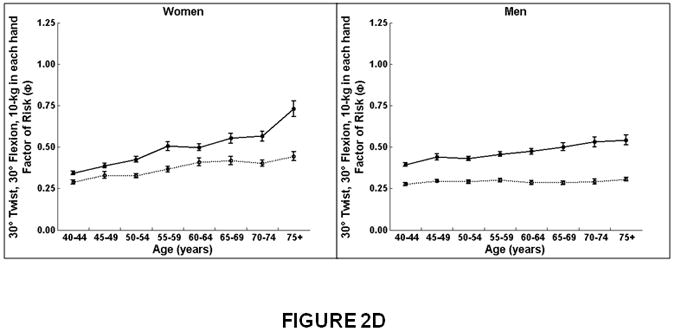
We used volumetric quantitative computed tomography (QCT) scans to evaluate volumetric bone density (vBMD), geometry, and strength in the thoracic (T8 to T10) and lumbar (L3 to L5) spine and determined how these parameters varied with age, sex, and spinal region. Participants included 690 participants of the Framingham Study, 40 to 87 years old (mean, 61 years). In both women and men, trabecular vBMD declined with age similarly for lumbar and thoracic regions, whereas cortical vBMD and integral vBMD, vertebral strength, and compressive force declined more at the lumbar spine than thoracic spine (interaction, p < 0.01). Notably, in men, cortical vBMD increased (β = 0.0004, p = 0.01), and vertebral strength did not change (β = 1.9305, p = 0.66) at the thoracic spine with age. In both women and men, vertebral cross-sectional area increased less and the factor-of-risk increased more with age at the lumbar than at the thoracic region (interaction, p < 0.01). For example, in women, the factor-of-risk for forward flexion increased (worsened) with age 6.8-fold more in the lumbar spine (β = 0.0157), compared with the thoracic spine (β = 0.0023). vBMD and vertebral strength declined more and the factor-of-risk increased more with age in women than men (interaction, p < 0.01). For instance, integral vBMD for the lumbar spine declined 36% from 40 to 75 years of age in women compared with 18% in men. There was little or no age-related change in the forces applied to the thoracic vertebrae in either women or men. Age-related changes were greater in the lumbar spine than in the thoracic region and greater in women than men. Whereas women lost bone density and strength at both the thoracic and lumbar spine, in men, vertebral strength declined only at the lumbar spine. Our study confirms the importance of evaluating determinants of vertebral strength in both the thoracic and lumbar spine and in both women and men to understand mechanisms underlying the structural failure of vertebral bodies with aging.
© 2012 American Society for Bone and Mineral Research
Figures
Similar articles
-
Bone density and strength from thoracic and lumbar CT scans both predict incident vertebral fractures independently of fracture location.Osteoporos Int. 2021 Feb;32(2):261-269. doi: 10.1007/s00198-020-05528-4. Epub 2020 Aug 3. Osteoporos Int. 2021. PMID: 32748310 Free PMC article.
-
Cervicothoracic volumetric bone mineral density assessed by opportunistic QCT may be a reliable marker for osteoporosis in adults.Osteoporos Int. 2025 Mar;36(3):423-433. doi: 10.1007/s00198-024-07373-1. Epub 2024 Dec 31. Osteoporos Int. 2025. PMID: 39738830 Free PMC article.
-
Mechanical contributions of the cortical and trabecular compartments contribute to differences in age-related changes in vertebral body strength in men and women assessed by QCT-based finite element analysis.J Bone Miner Res. 2011 May;26(5):974-83. doi: 10.1002/jbmr.287. J Bone Miner Res. 2011. PMID: 21542000 Free PMC article.
-
Vertebral size, bone density, and strength in men and women matched for age and areal spine BMD.J Bone Miner Res. 2014 Mar;29(3):562-9. doi: 10.1002/jbmr.2067. J Bone Miner Res. 2014. PMID: 23955966 Free PMC article.
-
Does thoracic or lumbar spine bone architecture predict vertebral failure strength more accurately than density?Osteoporos Int. 2008 Apr;19(4):537-45. doi: 10.1007/s00198-007-0478-x. Epub 2007 Oct 3. Osteoporos Int. 2008. PMID: 17912574
Cited by
-
Evaluation of a new approach to compute intervertebral disc height measurements from lateral radiographic views of the spine.Eur Spine J. 2017 Jan;26(1):167-172. doi: 10.1007/s00586-016-4817-5. Epub 2016 Oct 18. Eur Spine J. 2017. PMID: 27757680 Free PMC article.
-
Spinal Loading Patterns From Biomechanical Modeling Explain the High Incidence of Vertebral Fractures in the Thoracolumbar Region.J Bone Miner Res. 2017 Jun;32(6):1282-1290. doi: 10.1002/jbmr.3113. Epub 2017 Mar 28. J Bone Miner Res. 2017. PMID: 28244135 Free PMC article.
-
Prognostic value of preoperative low bone mineral density in patients with digestive cancers: a systematic review and meta-analysis.Arch Osteoporos. 2022 Feb 11;17(1):33. doi: 10.1007/s11657-022-01060-6. Arch Osteoporos. 2022. PMID: 35149903 Free PMC article.
-
A Longitudinal Study of Trunk Muscle Properties and Severity of Thoracic Kyphosis in Women and Men: The Framingham Study.J Gerontol A Biol Sci Med Sci. 2019 Feb 15;74(3):420-427. doi: 10.1093/gerona/gly056. J Gerontol A Biol Sci Med Sci. 2019. PMID: 29688268 Free PMC article.
-
Sex differences and age-related changes in vertebral body volume and volumetric bone mineral density at the thoracolumbar spine using opportunistic QCT.Front Endocrinol (Lausanne). 2024 Feb 15;15:1352048. doi: 10.3389/fendo.2024.1352048. eCollection 2024. Front Endocrinol (Lausanne). 2024. PMID: 38440788 Free PMC article.
References
-
- Melton LJd, Lane AW, Cooper C, Eastell R, O'Fallon WM, Riggs BL. Prevalence and incidence of vertebral deformities. Osteoporos Int. 1993;3(3):113–9. - PubMed
-
- Bone Health and Osteoporosis: A Report of the Surgeon General. US Department of Health and Human Services, Office of the Surgeon General; Rockville, MD: 2004. - PubMed
-
- Delmas PD, van de Langerijt L, Watts NB, Eastell R, Genant H, Grauer A, Cahall DL. Underdiagnosis of vertebral fractures is a worldwide problem: the IMPACT study. J Bone Miner Res. 2005;20(4):557–63. - PubMed
-
- Cauley JA, Hochberg MC, Lui LY, Palermo L, Ensrud KE, Hillier TA, Nevitt MC, Cummings SR. Long-term risk of incident vertebral fractures. Jama. 2007;298(23):2761–7. - PubMed
-
- Samelson EJ, Hannan MT, Zhang Y, Genant HK, Felson DT, Kiel DP. Incidence and risk factors for vertebral fracture in women and men: 25-year follow-up results from the population-based Framingham study. J Bone Miner Res. 2006;21(8):1207–14. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
