

Long-term effects of changes in cardiorespiratory fitness and body mass index on all-cause and cardiovascular disease mortality in men: the Aerobics Center Longitudinal Study
- PMID: 22144631
- PMCID: PMC3238382
- DOI: 10.1161/CIRCULATIONAHA.111.038422
Long-term effects of changes in cardiorespiratory fitness and body mass index on all-cause and cardiovascular disease mortality in men: the Aerobics Center Longitudinal Study
Abstract
Background: The combined associations of changes in cardiorespiratory fitness and body mass index (BMI) with mortality remain controversial and uncertain.
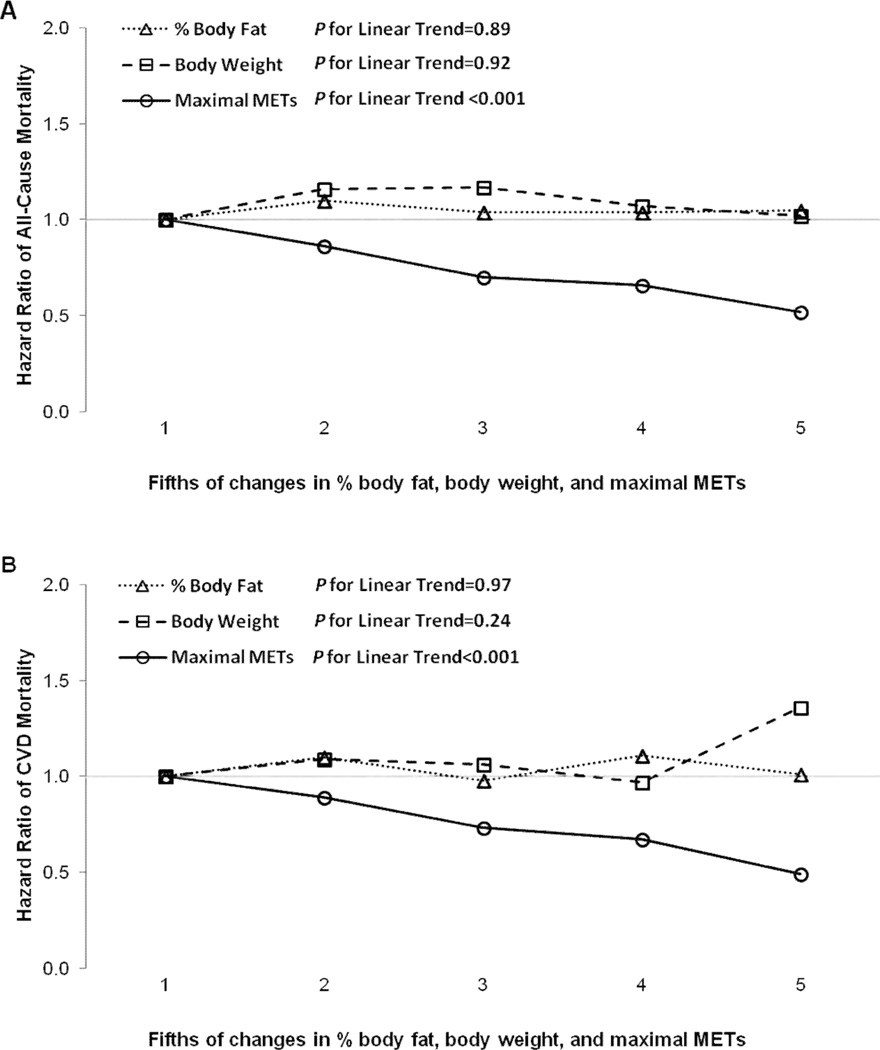
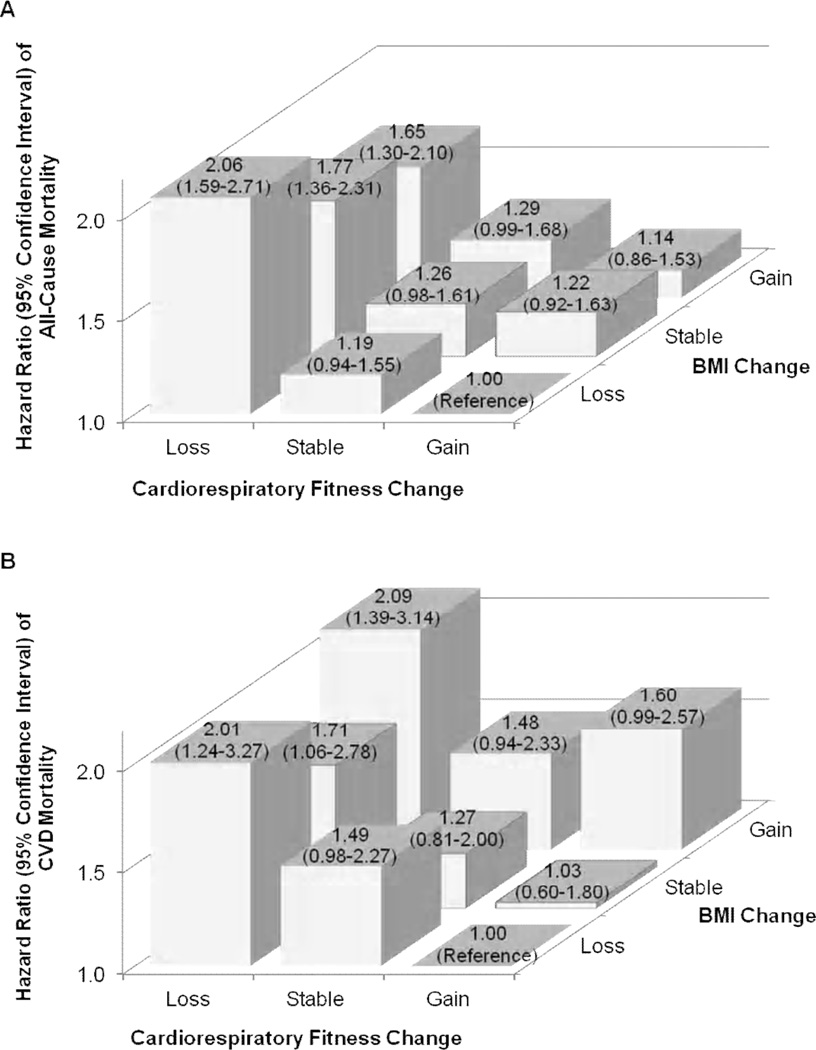
Methods and results: We examined the independent and combined associations of changes in fitness and BMI with all-cause and cardiovascular disease (CVD) mortality in 14 345 men (mean age 44 years) with at least 2 medical examinations. Fitness, in metabolic equivalents (METs), was estimated from a maximal treadmill test. BMI was calculated using measured weight and height. Changes in fitness and BMI between the baseline and last examinations over 6.3 years were classified into loss, stable, or gain groups. During 11.4 years of follow-up after the last examination, 914 all-cause and 300 CVD deaths occurred. The hazard ratios (95% confidence intervals) of all-cause and CVD mortality were 0.70 (0.59-0.83) and 0.73 (0.54-0.98) for stable fitness, and 0.61 (0.51-0.73) and 0.58 (0.42-0.80) for fitness gain, respectively, compared with fitness loss in multivariable analyses including BMI change. Every 1-MET improvement was associated with 15% and 19% lower risk of all-cause and CVD mortality, respectively. BMI change was not associated with all-cause or CVD mortality after adjusting for possible confounders and fitness change. In the combined analyses, men who lost fitness had higher all-cause and CVD mortality risks regardless of BMI change.
Conclusions: Maintaining or improving fitness is associated with a lower risk of all-cause and CVD mortality in men. Preventing age-associated fitness loss is important for longevity regardless of BMI change.
Figures
Similar articles
-
Association of changes in fitness and body composition with cancer mortality in men.Med Sci Sports Exerc. 2014 Jul;46(7):1366-74. doi: 10.1249/MSS.0000000000000225. Med Sci Sports Exerc. 2014. PMID: 24276414 Free PMC article.
-
A non-exercise testing method for estimating cardiorespiratory fitness: associations with all-cause and cardiovascular mortality in a pooled analysis of eight population-based cohorts.Eur Heart J. 2013 Mar;34(10):750-8. doi: 10.1093/eurheartj/ehs097. Epub 2012 May 3. Eur Heart J. 2013. PMID: 22555215 Free PMC article.
-
Longitudinal algorithms to estimate cardiorespiratory fitness: associations with nonfatal cardiovascular disease and disease-specific mortality.J Am Coll Cardiol. 2014 Jun 3;63(21):2289-96. doi: 10.1016/j.jacc.2014.03.008. Epub 2014 Apr 2. J Am Coll Cardiol. 2014. PMID: 24703924 Free PMC article.
-
Fitness vs. fatness on all-cause mortality: a meta-analysis.Prog Cardiovasc Dis. 2014 Jan-Feb;56(4):382-90. doi: 10.1016/j.pcad.2013.09.002. Epub 2013 Oct 11. Prog Cardiovasc Dis. 2014. PMID: 24438729 Review.
-
The Joint Association of Fitness and Fatness on Cardiovascular Disease Mortality: A Meta-Analysis.Prog Cardiovasc Dis. 2018 Jul-Aug;61(2):136-141. doi: 10.1016/j.pcad.2018.07.004. Epub 2018 Jul 5. Prog Cardiovasc Dis. 2018. PMID: 29981352 Review.
Cited by
-
Leisure-time physical activity and mortality in a multiethnic prospective cohort study: the Northern Manhattan Study.Ann Epidemiol. 2015 Jul;25(7):475-479.e2. doi: 10.1016/j.annepidem.2015.04.001. Epub 2015 Apr 18. Ann Epidemiol. 2015. PMID: 25982960 Free PMC article.
-
Do changes in frailty, physical functioning, and cognitive functioning predict mortality in old age? Results from the Longitudinal Aging Study Amsterdam.BMC Geriatr. 2022 Mar 12;22(1):193. doi: 10.1186/s12877-022-02876-0. BMC Geriatr. 2022. PMID: 35279092 Free PMC article.
-
Physical Activity and Type 2 Diabetes: In Search of a Personalized Approach to Improving β-Cell Function.Nutrients. 2023 Sep 28;15(19):4202. doi: 10.3390/nu15194202. Nutrients. 2023. PMID: 37836486 Free PMC article. Review.
-
Exercise Training Combined with Calanus Oil Supplementation Improves the Central Cardiodynamic Function in Older Women.Nutrients. 2021 Dec 29;14(1):149. doi: 10.3390/nu14010149. Nutrients. 2021. PMID: 35011022 Free PMC article.
-
Time-efficient and computer-guided sprint interval exercise training for improving health in the workplace: a randomised mixed-methods feasibility study in office-based employees.BMC Public Health. 2020 Mar 12;20(1):313. doi: 10.1186/s12889-020-8444-z. BMC Public Health. 2020. PMID: 32164631 Free PMC article. Clinical Trial.
References
-
- Gulati M, Black HR, Shaw LJ, Arnsdorf MF, Merz CN, Lauer MS, Marwick TH, Pandey DK, Wicklund RH, Thisted RA. The prognostic value of a nomogram for exercise capacity in women. N Engl J Med. 2005;353:468–475. - PubMed
-
- Kodama S, Saito K, Tanaka S, Maki M, Yachi Y, Asumi M, Sugawara A, Totsuka K, Shimano H, Ohashi Y, Yamada N, Sone H. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA. 2009;301:2024–2035. - PubMed
-
- Myers J, Prakash M, Froelicher V, Do D, Partington S, Atwood JE. Exercise capacity and mortality among men referred for exercise testing. N Engl J Med. 2002;346:793–801. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
