

Experimental subarachnoid hemorrhage causes early and long-lasting microarterial constriction and microthrombosis: an in-vivo microscopy study
- PMID: 22146194
- PMCID: PMC3293113
- DOI: 10.1038/jcbfm.2011.154
Experimental subarachnoid hemorrhage causes early and long-lasting microarterial constriction and microthrombosis: an in-vivo microscopy study
Abstract
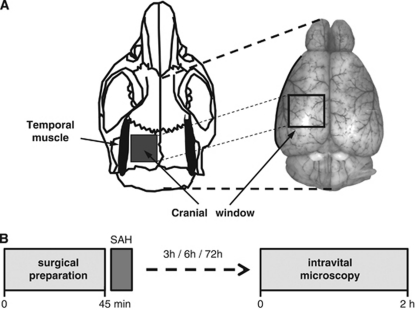
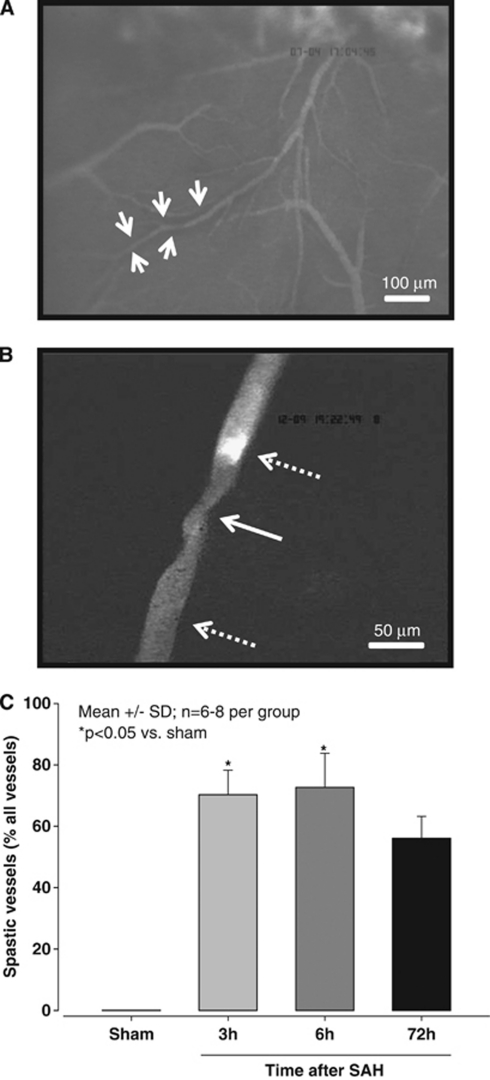
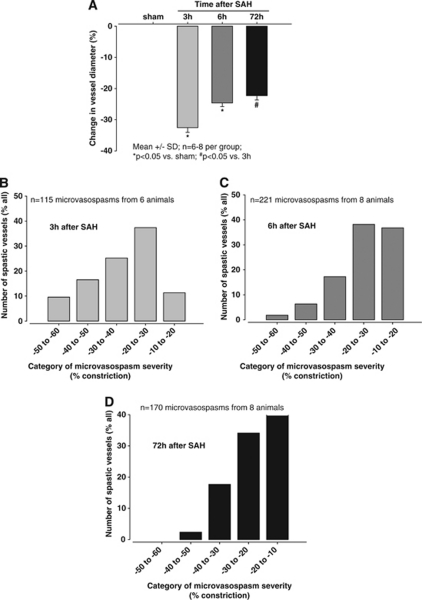
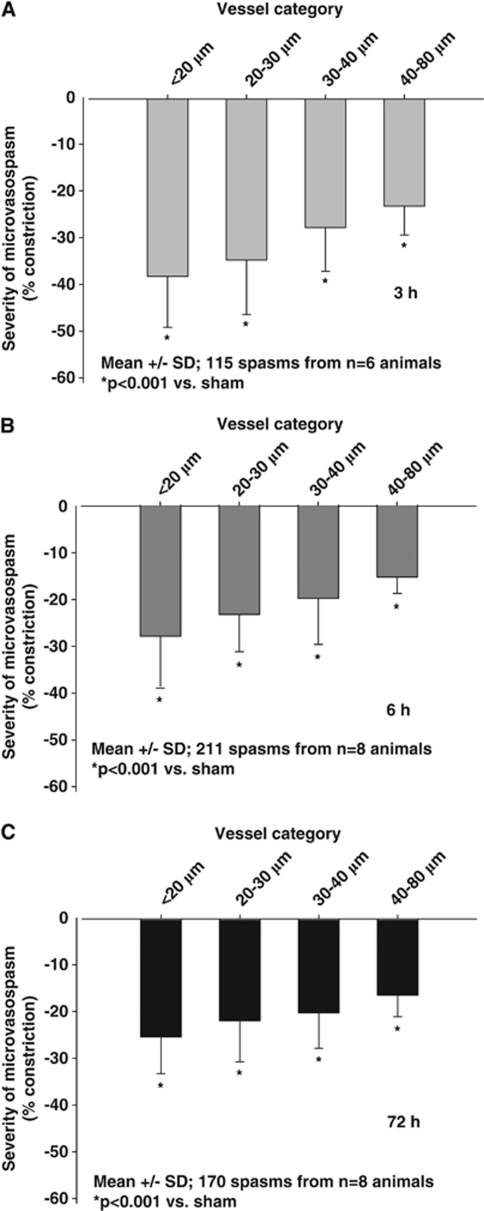
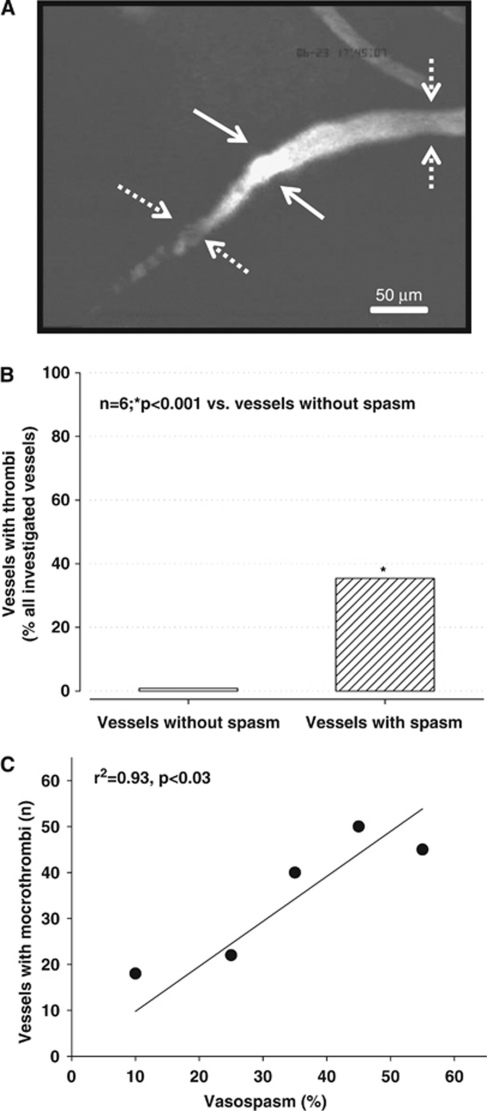
Early brain injury (EBI) after subarachnoid hemorrhage (SAH) is characterized by a severe, cerebral perfusion pressure (CPP)-independent reduction in cerebral blood flow suggesting alterations on the level of cerebral microvessels. Therefore, we aimed to use in-vivo imaging to investigate the cerebral microcirculation after experimental SAH. Subarachnoid hemorrhage was induced in C57/BL6 mice by endovascular perforation. Pial arterioles and venules (10 to 80 μm diameter) were examined using in-vivo fluorescence microscopy, 3, 6, and 72 hours after SAH. Venular diameter or flow was not affected by SAH, while >70% of arterioles constricted by 22% to 33% up to 3 days after hemorrhage (P<0.05 versus sham). The smaller the investigated arterioles, the more pronounced the constriction (r(2)=0.92, P<0.04). Approximately 30% of constricted arterioles were occluded by microthrombi and the frequency of arteriolar microthrombosis correlated with the degree of constriction (r(2)=0.93, P<0.03). The current study demonstrates that SAH induces microarterial constrictions and microthrombosis in vivo. These findings may explain the early CPP-independent decrease in cerebral blood flow after SAH and may therefore serve as novel targets for the treatment of early perfusion deficits after SAH.
Figures
Similar articles
-
CO2 has no therapeutic effect on early microvasospasm after experimental subarachnoid hemorrhage.J Cereb Blood Flow Metab. 2014 Aug;34(8):e1-6. doi: 10.1038/jcbfm.2014.96. Epub 2014 May 28. J Cereb Blood Flow Metab. 2014. PMID: 24865999 Free PMC article.
-
Dynamic alterations of cerebral pial microcirculation during experimental subarachnoid hemorrhage.Cell Mol Neurobiol. 2009 Mar;29(2):235-41. doi: 10.1007/s10571-008-9316-8. Epub 2008 Sep 27. Cell Mol Neurobiol. 2009. PMID: 18821009 Free PMC article.
-
Temporal profile of thrombogenesis in the cerebral microcirculation after traumatic brain injury in mice.J Neurotrauma. 2010 Jan;27(1):121-30. doi: 10.1089/neu.2009.1114. J Neurotrauma. 2010. PMID: 19803784
-
The role of arterioles and the microcirculation in the development of vasospasm after aneurysmal SAH.Biomed Res Int. 2014;2014:253746. doi: 10.1155/2014/253746. Epub 2014 May 11. Biomed Res Int. 2014. PMID: 24900959 Free PMC article. Review.
-
Subarachnoid hemorrhage: a review of experimental studies on the microcirculation and the neurovascular unit.Transl Stroke Res. 2014 Apr;5(2):174-89. doi: 10.1007/s12975-014-0323-4. Epub 2014 Feb 11. Transl Stroke Res. 2014. PMID: 24510780 Review.
Cited by
-
Longitudinal imaging and evaluation of SAH-associated cerebral large artery vasospasm in mice using micro-CT and angiography.J Cereb Blood Flow Metab. 2020 Nov;40(11):2265-2277. doi: 10.1177/0271678X19887052. Epub 2019 Nov 21. J Cereb Blood Flow Metab. 2020. PMID: 31752586 Free PMC article.
-
CO2 has no therapeutic effect on early microvasospasm after experimental subarachnoid hemorrhage.J Cereb Blood Flow Metab. 2014 Aug;34(8):e1-6. doi: 10.1038/jcbfm.2014.96. Epub 2014 May 28. J Cereb Blood Flow Metab. 2014. PMID: 24865999 Free PMC article.
-
Nitric oxide inhalation reduces brain damage, prevents mortality, and improves neurological outcome after subarachnoid hemorrhage by resolving early pial microvasospasms.J Cereb Blood Flow Metab. 2016 Dec;36(12):2096-2107. doi: 10.1177/0271678X15605848. Epub 2015 Nov 2. J Cereb Blood Flow Metab. 2016. PMID: 26661144 Free PMC article.
-
Failed Neuroprotection of Combined Inhibition of L-Type and ASIC1a Calcium Channels with Nimodipine and Amiloride.Int J Mol Sci. 2020 Nov 24;21(23):8921. doi: 10.3390/ijms21238921. Int J Mol Sci. 2020. PMID: 33255506 Free PMC article.
-
Update: Microdialysis for Monitoring Cerebral Metabolic Dysfunction after Subarachnoid Hemorrhage.J Clin Med. 2020 Dec 30;10(1):100. doi: 10.3390/jcm10010100. J Clin Med. 2020. PMID: 33396652 Free PMC article. Review.
References
-
- Adams HP, Jr, Kassell NF, Torner JC, Nibbelink DW, Sahs AL. Early management of aneurysmal subarachnoid hemorrhage. A report of the Cooperative Aneurysm Study. J Neurosurg. 1981;54:141–145. - PubMed
-
- Bederson JB, Germano IM, Guarino L. Cortical blood flow and cerebral perfusion pressure in a new noncraniotomy model of subarachnoid hemorrhage in the rat. Stroke. 1995;26:1086–1091. - PubMed
-
- Bederson JB, Levy AL, Ding WH, Kahn R, DiPerna CA, Jenkins AL, III, Vallabhajosyula P. Acute vasoconstriction after subarachnoid hemorrhage. Neurosurgery. 1998;42:352–360. - PubMed
-
- Feiler S, Friedrich B, Schöller K, Thal SC, Plesnila N. Standardized induction of subarachnoid hemorrhage in mice by intracranial pressure monitoring. J Neurosci Methods. 2010;190:164–170. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
