

Early cognitive function, recovery and well-being after sevoflurane and xenon anaesthesia in the elderly: a double-blinded randomized controlled trial
- PMID: 22146537
- PMCID: PMC3231879
- DOI: 10.1186/2045-9912-1-9
Early cognitive function, recovery and well-being after sevoflurane and xenon anaesthesia in the elderly: a double-blinded randomized controlled trial
Abstract
Background: The postoperative cognitive function is impaired in elderly patients after general anaesthesia. The fast recovery after xenon anaesthesia was hypothesized to be advantageous in this scenario. We compared early postoperative cognitive function after xenon and sevoflurane anaesthesia in this study.
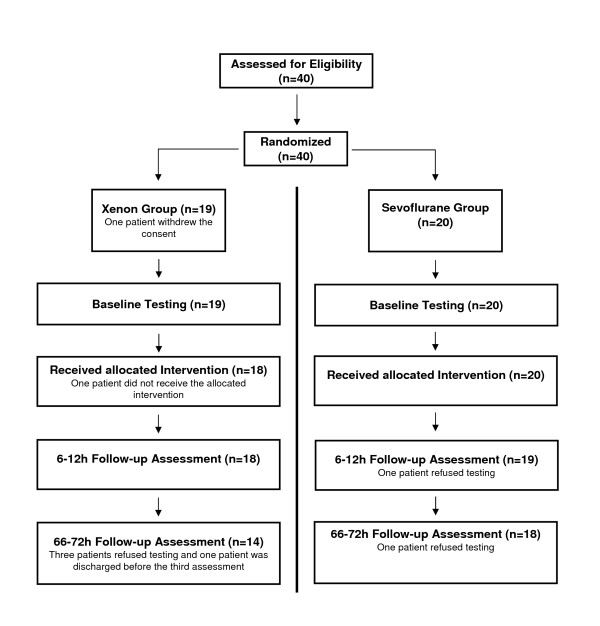
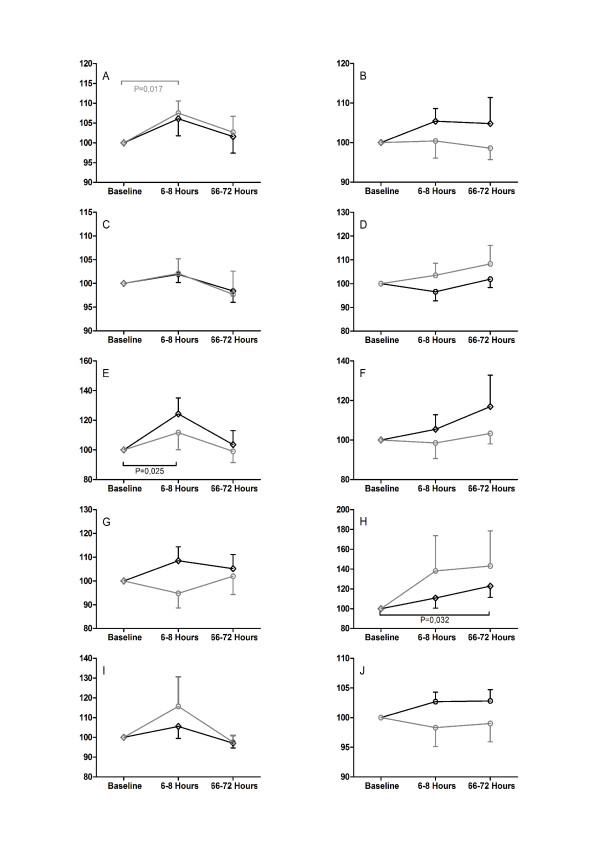
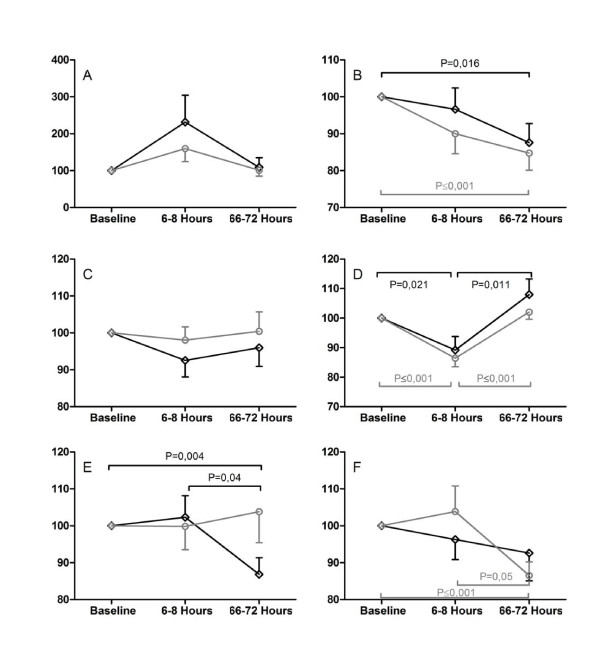
Methods: The study was approved by the local ethics committee and written informed consent was obtained from each patient. Patients aged 65-75 years (ASA I-III) scheduled for elective surgery (duration 60-180 min) were enrolled. Investigators performing cognitive testing and patients were blinded towards allocation to either xenon or sevoflurane anaesthesia. Baseline assessment of cognitive function was carried out 12-24 h before the operation. The results were compared to follow-up tests 6-12 and 66-72 h after surgery. Primary outcome parameter was the subtest "Alertness" of the computerized Test of Attentional Performance (TAP). Secondary outcome parameters included further subtests of the TAP, several Paper-Pencil-Tests, emergence times from anaesthesia, modified Aldrete scores and patients' well-being.
Results: 40 patients were randomized and equally allocated to both groups. No significant differences were found in the TAP or the Paper-Pencil-Tests at 6-12 and 66-72 h after the operation. All emergence times were faster after xenon anaesthesia. The modified Aldrete scores were significantly higher during the first hour in the xenon group. No difference in well-being could be detected between both groups.
Conclusions: The results show no difference in the incidence of postoperative cognitive dysfunction (POCD) after xenon or sevoflurane anaesthesia. Emergence from general anaesthesia was faster in the xenon group.
Figures
Similar articles
-
Emergence and early cognitive function in the elderly after xenon or desflurane anaesthesia: a double-blinded randomized controlled trial.Br J Anaesth. 2007 Jun;98(6):756-62. doi: 10.1093/bja/aem103. Epub 2007 May 7. Br J Anaesth. 2007. PMID: 17485435 Clinical Trial.
-
Comparison of early cognitive function and recovery after desflurane or sevoflurane anaesthesia in the elderly: a double-blinded randomized controlled trial.Br J Anaesth. 2010 Feb;104(2):167-74. doi: 10.1093/bja/aep369. Epub 2009 Dec 30. Br J Anaesth. 2010. PMID: 20042477 Clinical Trial.
-
Evaluation of bispectral index and auditory evoked potentials for hypnotic depth monitoring during balanced xenon anaesthesia compared with sevoflurane.Br J Anaesth. 2010 Sep;105(3):334-41. doi: 10.1093/bja/aeq163. Epub 2010 Jul 14. Br J Anaesth. 2010. PMID: 20630890 Clinical Trial.
-
The hip fracture surgery in elderly patients (HIPELD) study to evaluate xenon anaesthesia for the prevention of postoperative delirium: a multicentre, randomized clinical trial.Br J Anaesth. 2018 Jan;120(1):127-137. doi: 10.1016/j.bja.2017.11.015. Epub 2017 Nov 21. Br J Anaesth. 2018. PMID: 29397119 Clinical Trial.
-
Sevoflurane. A review of its pharmacodynamic and pharmacokinetic properties and its clinical use in general anaesthesia.Drugs. 1996 Apr;51(4):658-700. doi: 10.2165/00003495-199651040-00009. Drugs. 1996. PMID: 8706599 Review.
Cited by
-
Safety and feasibility of xenon as an adjuvant to sevoflurane anaesthesia in children undergoing interventional or diagnostic cardiac catheterization: study protocol for a randomised controlled trial.Trials. 2015 Mar 4;16:74. doi: 10.1186/s13063-015-0587-3. Trials. 2015. PMID: 25886748 Free PMC article. Clinical Trial.
-
Postoperative Cognitive Dysfunction.Indian J Crit Care Med. 2019 Jun;23(Suppl 2):S162-S164. doi: 10.5005/jp-journals-10071-23196. Indian J Crit Care Med. 2019. PMID: 31485127 Free PMC article. Review.
-
Noble gas and neuroprotection: From bench to bedside.Front Pharmacol. 2022 Nov 29;13:1028688. doi: 10.3389/fphar.2022.1028688. eCollection 2022. Front Pharmacol. 2022. PMID: 36532733 Free PMC article. Review.
-
Xenon for the prevention of postoperative delirium in cardiac surgery: study protocol for a randomized controlled clinical trial.Trials. 2015 Oct 9;16:449. doi: 10.1186/s13063-015-0987-4. Trials. 2015. PMID: 26452540 Free PMC article. Clinical Trial.
-
Short-term inhalation of xenon during anesthesia for prevention of postoperative delirium in elderly patients undergoing laparoscopic radical colectomy: study protocol for a randomized controlled clinical trial.Trials. 2024 Jul 2;25(1):434. doi: 10.1186/s13063-024-08290-8. Trials. 2024. PMID: 38956691 Free PMC article.
References
-
- Moller JT, Cluitmans P, Rasmussen LS, Houx P, Rasmussen H, Canet J, Rabbitt P, Jolles J, Larsen K, Hanning CD, Langeron O, Johnson T, Lauven PM, Kristensen PA, Biedler A, van Beem H, Fraidakis O, Silverstein JH, Beneken JE, Gravenstein JS. Long-term postoperative cognitive dysfunction in the elderly: ISPOCD1 study. Lancet. 1998;351:857–861. doi: 10.1016/S0140-6736(97)07382-0. - DOI - PubMed
-
- Wappler F, Rossaint R, Baumert J, Scholz J, Tonner PH, van Aken H, Berendes E, Klein J, Gommers D, Hammerle A, Franke A, Hofmann T, Schulte Esch J. Multicenter randomized comparison of xenon and isoflurane on left ventricular function in patients undergoing elective surgery. Anesthesiology. 2007;106:463–471. doi: 10.1097/00000542-200703000-00010. - DOI - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
