

Updated report on comparative effectiveness of ACE inhibitors, ARBs, and direct renin inhibitors for patients with essential hypertension: much more data, little new information
- PMID: 22147122
- PMCID: PMC3358398
- DOI: 10.1007/s11606-011-1938-8
Updated report on comparative effectiveness of ACE inhibitors, ARBs, and direct renin inhibitors for patients with essential hypertension: much more data, little new information
Abstract
Objectives: A 2007 systematic review compared angiotensin-converting enzyme (ACE) inhibitors and angiotensin II receptor blockers (ARBs) in patients with hypertension. Direct renin inhibitors (DRIs) have since been introduced, and significant new research has been published. We sought to update and expand the 2007 review.
Data sources: We searched MEDLINE and EMBASE (through December 2010) and selected other sources for relevant English-language trials.
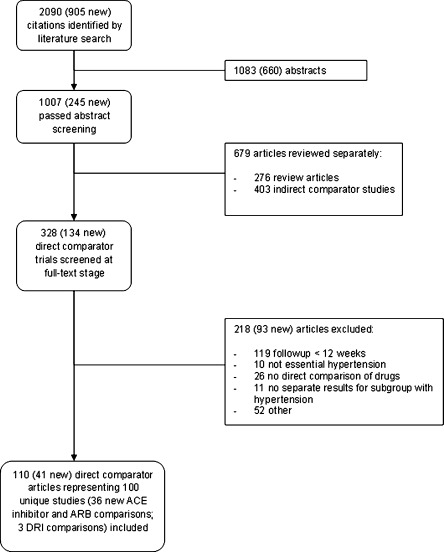
Study eligibility criteria, participants, and interventions: We included studies that directly compared ACE inhibitors, ARBs, and/or DRIs in at least 20 total adults with essential hypertension; had at least 12 weeks of follow-up; and reported at least one outcome of interest. Ninety-seven (97) studies (36 new since 2007) directly comparing ACE inhibitors versus ARBs and three studies directly comparing DRIs to ACE inhibitor inhibitors or ARBs were included.
Study appraisal and synthesis methods: A standard protocol was used to extract data on study design, interventions, population characteristics, and outcomes; evaluate study quality; and summarize the evidence.
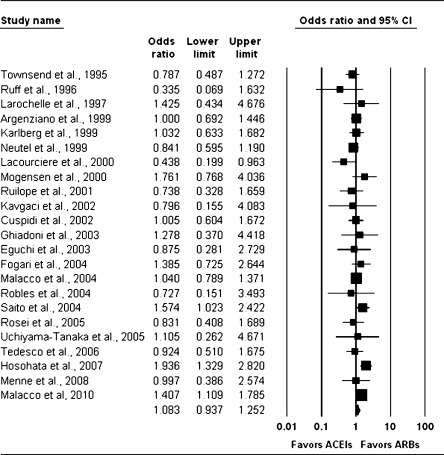
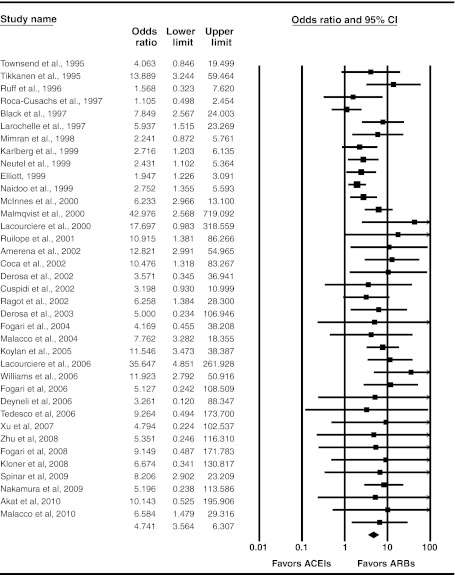
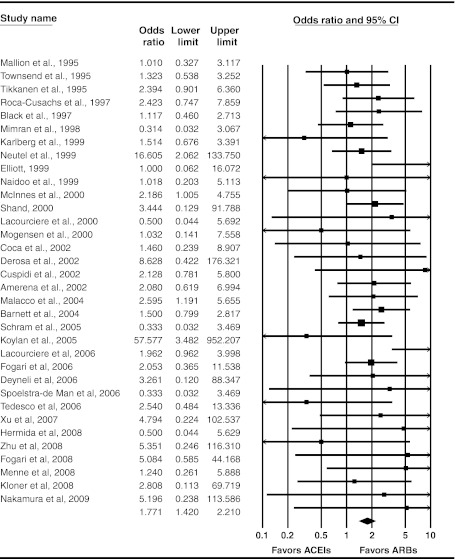
Results: In spite of substantial new evidence, none of the conclusions from the 2007 review changed. The level of evidence remains high for equivalence between ACE inhibitors and ARBs for blood pressure lowering and use as single antihypertensive agents, as well as for superiority of ARBs for short-term adverse events (primarily cough). However, the new evidence was insufficient on long-term cardiovascular outcomes, quality of life, progression of renal disease, medication adherence or persistence, rates of angioedema, and differences in key patient subgroups.
Limitations: Included studies were limited by follow-up duration, protocol heterogeneity, and infrequent reporting on patient subgroups.
Conclusions and implications of key findings: Evidence does not support a meaningful difference between ACE inhibitors and ARBs for any outcome except medication side effects. Few, if any, of the questions that were not answered in the 2007 report have been addressed by the 36 new studies. Future research in this area should consider areas of uncertainty and be prioritized accordingly.
Figures
Comment in
-
Newer is not always better: all antihypertensive medications do not equally reduce cardiovascular risk.J Gen Intern Med. 2012 Jun;27(6):618-20. doi: 10.1007/s11606-012-2020-x. J Gen Intern Med. 2012. PMID: 22382456 Free PMC article. No abstract available.
-
ACE inhibitors versus ARBs versus DRIs: a systematic update.J Gen Intern Med. 2012 Dec;27(12):1585; author reply 1586. doi: 10.1007/s11606-012-2212-4. J Gen Intern Med. 2012. PMID: 22965670 Free PMC article. No abstract available.
-
Comparative effectiveness of renin-angiotensin system inhibitors in hypertension.J Comp Eff Res. 2012 Mar;1(2):125-7. doi: 10.2217/cer.12.2. J Comp Eff Res. 2012. PMID: 24237372
References
-
- Lewington S, Clarke R, Qizilbash N, et al. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies.[Erratum appears in Lancet. 2003 Mar 22;361(9362):1060] Lancet. 2002;360(9349):1903–1913. doi: 10.1016/S0140-6736(02)11911-8. - DOI - PubMed
-
- Matchar DB, McCrory DC, Orlando LA, et al. Comparative Effectiveneness of Angiotensin-Converting Enzyme Inhibitors (ACEIs) and Angiotensin II Receptor Antagonists (ARBs) for Treating Essential Hypertension. Comparative Effectiveness Review No. 10. (Prepared by Duke Evidence-based Practice Center under Contract No. 290-02-0025.) Rockville, MD: Agency for Healthcare Research and Quality. November 2007. Available at: www.effectivehealthcare.ahrq.gov/reports/final.cfm. Accessed October 31, 2010. - PubMed
-
- Matchar DB, McCrory DC, Orlando LA, et al. Systematic review: comparative effectiveness of angiotensin-converting enzyme inhibitors and angiotensin II receptor blockers for treating essential hypertension. Ann Intern Med. 2008;148(1):16–29. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
