

Cost-effectiveness of different screening strategies for osteoporosis in postmenopausal women
- PMID: 22147714
- PMCID: PMC3318923
- DOI: 10.7326/0003-4819-155-11-201112060-00007
Cost-effectiveness of different screening strategies for osteoporosis in postmenopausal women
Abstract
Background: The best strategies to screen postmenopausal women for osteoporosis are not clear.
Objective: To identify the cost-effectiveness of various screening strategies.
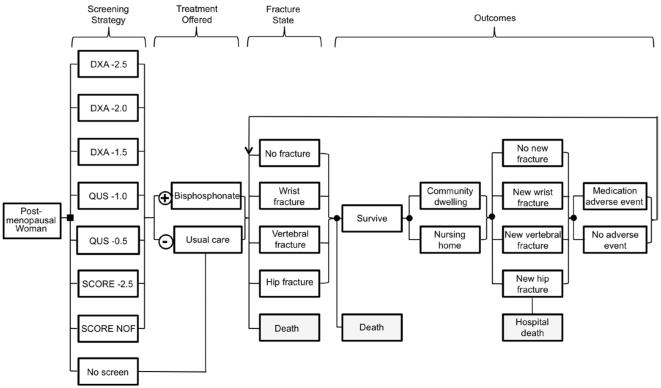
Design: Individual-level state-transition cost-effectiveness model.
Data sources: Published literature.
Target population: U.S. women aged 55 years or older.
Time horizon: Lifetime.
Perspective: Payer.
Intervention: Screening strategies composed of alternative tests (central dual-energy x-ray absorptiometry [DXA], calcaneal quantitative ultrasonography [QUS], and the Simple Calculated Osteoporosis Risk Estimation [SCORE] tool) initiation ages, treatment thresholds, and rescreening intervals. Oral bisphosphonate treatment was assumed, with a base-case adherence rate of 50% and a 5-year on/off treatment pattern.
Outcome measures: Incremental cost-effectiveness ratios (2010 U.S. dollars per quality-adjusted life-year [QALY] gained).
Results of base-case analysis: At all evaluated ages, screening was superior to not screening. In general, quality-adjusted life-days gained with screening tended to increase with age. At all initiation ages, the best strategy with an incremental cost-effectiveness ratio (ICER) of less than $50,000 per QALY was DXA screening with a T-score threshold of -2.5 or less for treatment and with follow-up screening every 5 years. Across screening initiation ages, the best strategy with an ICER less than $50,000 per QALY was initiation of screening at age 55 years by using DXA -2.5 with rescreening every 5 years. The best strategy with an ICER less than $100,000 per QALY was initiation of screening at age 55 years by using DXA with a T-score threshold of -2.0 or less for treatment and then rescreening every 10 years. No other strategy that involved treatment of women with osteopenia had an ICER less than $100,000 per QALY. Many other strategies, including strategies with SCORE or QUS prescreening, were also cost-effective, and in general the differences in effectiveness and costs between evaluated strategies was small.
Results of sensitivity analysis: Probabilistic sensitivity analysis did not reveal a consistently superior strategy.
Limitations: Data were primarily from white women. Screening initiation at ages younger than 55 years were not examined. Only osteoporotic fractures of the hip, vertebrae, and wrist were modeled.
Conclusion: Many strategies for postmenopausal osteoporosis screening are effective and cost-effective, including strategies involving screening initiation at age 55 years. No strategy substantially outperforms another.
Primary funding source: National Center for Research Resources.
Figures
Comment in
-
Comparative effectiveness and cost-effectiveness of strategies to screen for osteoporosis in postmenopausal women.Ann Intern Med. 2011 Dec 6;155(11):788-9. doi: 10.7326/0003-4819-155-11-201112060-00012. Ann Intern Med. 2011. PMID: 22147717 No abstract available.
-
Screening for postmenopausal osteoporosis with any modality is cost-effective including screening initiation at 55 years of age.Evid Based Med. 2012 Dec;17(6):195-6. doi: 10.1136/ebmed-2012-100779. Epub 2012 Jul 10. Evid Based Med. 2012. PMID: 22782917 No abstract available.
References
-
- National Osteoporosis Foundation . About Osteoporosis: Fast Facts. National Osteoporosis Foundation; Washington, DC: 2005.
-
- Nelson HD, Helfand M, Woolf SH, Allan JD. Screening for postmenopausal osteoporosis: a review of the evidence for the U.S. Preventive Services Task Force. Ann Intern Med. 2002;137:529–41. [PMID: 12230356] - PubMed
-
- Burge R, Dawson-Hughes B, Solomon DH, Wong JB, King A, Tosteson A. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005-2025. J Bone Miner Res. 2007;22:465–75. [PMID: 17144789] - PubMed
-
- U.S. Department of Health and Human Services . Bone Health and Osteoporosis: A Report of the Surgeon General. U.S. Department of Health and Human Services, Office of the Surgeon General; Rockville, MD: 2004.
-
- Liu H, Michaud K, Nayak S, Karpf DB, Owens DK, Garber AM. The cost-effectiveness of therapy with teriparatide and alendronate in women with severe osteoporosis. Arch Intern Med. 2006;166:1209–17. [PMID: 16772249] - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials