

Ten-year trends in quality of care and spending for depression: 1996 through 2005
- PMID: 22147841
- PMCID: PMC4876037
- DOI: 10.1001/archgenpsychiatry.2011.146
Ten-year trends in quality of care and spending for depression: 1996 through 2005
Abstract
Context: During the past decade, the introduction of generic versions of newer antidepressants and the release of Food and Drug Administration warnings regarding suicidality in children, adolescents, and young adults may have had an effect on cost and quality of depression treatment.
Objectives: To examine longitudinal trends in health service utilization, spending, and quality of care for depression.
Design: Observational trend study.
Setting: Florida Medicaid enrollees, between July 1, 1996, and June 30, 2006. Patients Annual cohorts aged 18 to 64 years diagnosed as having depression.
Main outcome measures: Mental health care spending (adjusted for inflation and case mix), as well as its components, including inpatient, outpatient, and medication expenditures. Quality-of-care measures included medication adherence, psychotherapy, and follow-up visits.
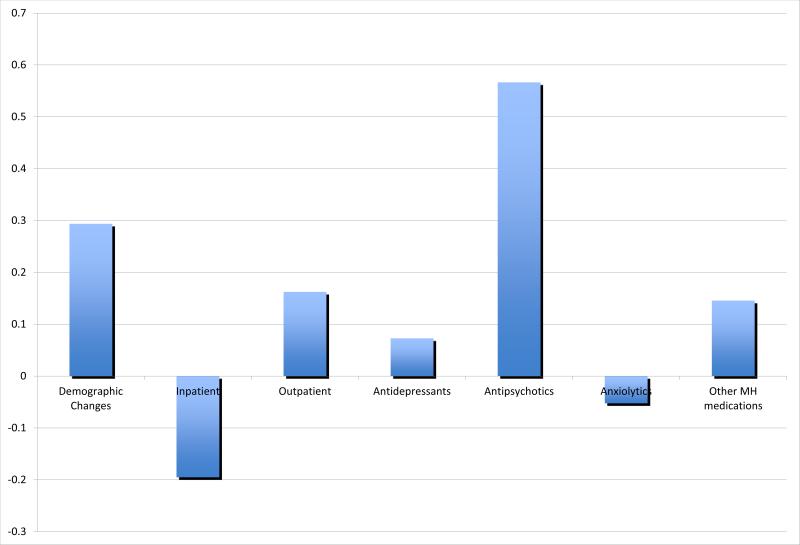
Results: Mental health care spending increased from a mean of $2802 per enrollee to $3610 during this period (29% increase). This increase occurred despite a mean decrease in inpatient spending from $641 per enrollee to $373 and was driven primarily by an increase in pharmacotherapy spending (up 110%), the bulk of which was due to spending on antipsychotics (949% increase). The percentage of enrollees with depression who were hospitalized decreased from 9.1% to 5.1%, and the percentage who received psychotherapy decreased from 56.6% to 37.5%. Antidepressant use increased from 80.6% to 86.8%, anxiety medication use was unchanged at 62.7% and 64.4%, and antipsychotic use increased from 25.9% to 41.9%. Changes in quality of care were mixed, with antidepressant use improving slightly, psychotherapy utilization fluctuating, and follow-up visits decreasing.
Conclusions: During a 10-year period, spending for Medicaid enrollees with depression increased substantially, with minimal improvements in quality of care. Antipsychotic use contributed significantly to the increase in spending, while contributing little to traditional measures of quality of care.
Figures
References
-
- Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE. Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593–602. - PubMed
-
- Murray CJL, Lopez AD. The Global Burden of Disease: A comprehensive assessment of mortality and disability from diseases, injuries, and risk factors in 1990 and projected to 2020. Harvard University Press; Cambridge, MA: 1996.
-
- Wells KB, Stewart A, Hays RD, Burnam A, Rogers W, Daniels M, Berry S, Greenfield S, Ware J. The functioning and well-being of depressed patients: results from the Medical Outcomes Study. JAMA. 1989;262(7):914–919. - PubMed
-
- Druss BG, Rosenheck RA, Sledge WH. Health and disability costs of depressive illness in a major U.S. corporation. Am J Psychiatry. 2000;157(8):1274–1278. - PubMed
-
- Simon GE, Von Korff M, Barlow W. Health care costs of primary care patients with recognized depression. Arch Gen Psychiatry. 1995;52(10):850–856. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
