

High-dose melphalan and peripheral blood stem cell transplantation for light-chain amyloidosis with cardiac involvement
- PMID: 22147893
- PMCID: PMC3277349
- DOI: 10.1182/blood-2011-07-370031
High-dose melphalan and peripheral blood stem cell transplantation for light-chain amyloidosis with cardiac involvement
Abstract
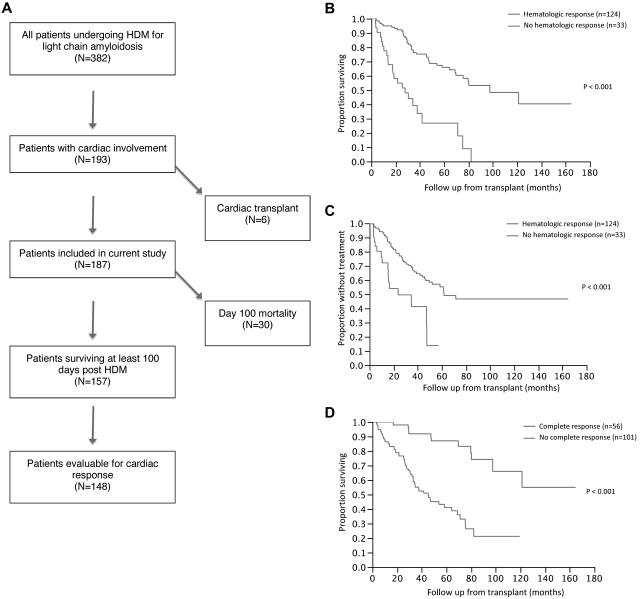
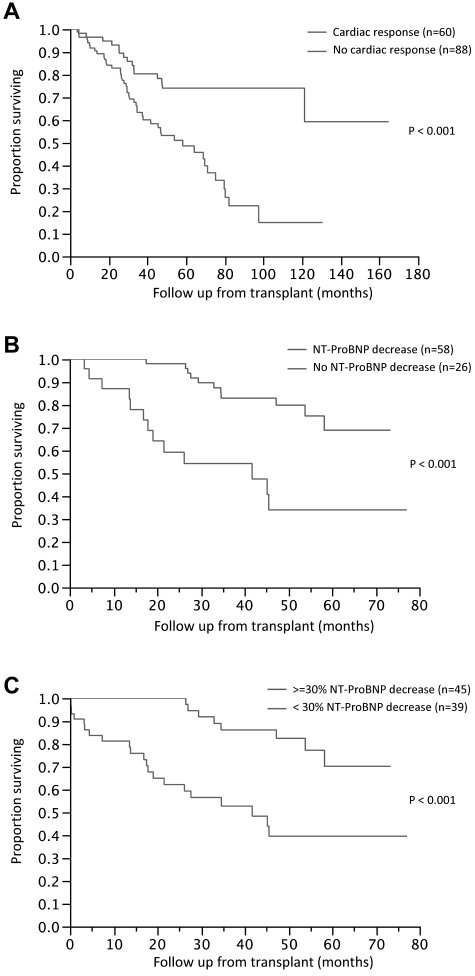
High-dose melphalan (HDM) plus stem cell transplantation is an effective treatment for light-chain amyloidosis (AL), but is associated with high treatment-related mortality in patients with cardiac involvement. We studied 187 patients with cardiac involvement with AL who underwent HDM between 1996 and 2008. The median age was 57 years and the median time from diagnosis to HDM was 3.6 months. Half of the patients received reduced-dose melphalan (100-160 mg/m(2)). The median overall survival (OS) was 66 months, 54 months from diagnosis and HDM, respectively, and 91 patients (49%) were alive at the last follow-up 52 months (median) from HDM. Thirty patients (16%) died within 100 days of transplantation; only low serum albumin predicted early deaths. Overall, hematologic response (HR) and cardiac responses were seen in 66% and 41% of patients, respectively. The median OS for patients with and without HR was not reached and 22 months, respectively (P < .01); and for those with any decrease and no decrease in N-terminal-pro-brain natriuretic peptide was not reached and 26 months, respectively (P < .01). In multivariate analysis of baseline factors, only reduced-dose melphalan predicted shorter OS. HDM is feasible in patients with cardiac amyloidosis, and achievement of HR and organ response is associated with improved survival.
Figures
Similar articles
-
Autologous stem cell transplantation for AL amyloidosis: adjustment of melphalan dose by factors including BNP.Int J Hematol. 2014 Dec;100(6):554-8. doi: 10.1007/s12185-014-1680-1. Epub 2014 Oct 4. Int J Hematol. 2014. PMID: 25281404
-
An overview of the use of high-dose melphalan with autologous stem cell transplantation for the treatment of AL amyloidosis.Bone Marrow Transplant. 2001 Oct;28(7):637-42. doi: 10.1038/sj.bmt.1703200. Bone Marrow Transplant. 2001. PMID: 11704785 Review.
-
Induction bortezomib in Al amyloidosis followed by high dose melphalan and autologous stem cell transplantation: a single institution retrospective study.Clin Lymphoma Myeloma Leuk. 2014 Oct;14(5):424-430.e1. doi: 10.1016/j.clml.2014.02.003. Epub 2014 Feb 16. Clin Lymphoma Myeloma Leuk. 2014. PMID: 24650974
-
Outcome of AL amyloidosis after high-dose melphalan and autologous stem cell transplantation: long-term results in a series of 421 patients.Blood. 2011 Oct 20;118(16):4346-52. doi: 10.1182/blood-2011-01-330738. Epub 2011 Aug 9. Blood. 2011. PMID: 21828140 Free PMC article.
-
High-Dose Melphalan and Autologous Peripheral Blood Stem Cell Transplantation in AL Amyloidosis.Acta Haematol. 2020;143(4):381-387. doi: 10.1159/000506498. Epub 2020 Apr 3. Acta Haematol. 2020. PMID: 32248194 Review.
Cited by
-
Incidental Extracardiac Findings of Technetium-99m Pyrophosphate Scintigraphy: A Pictorial Review.Cureus. 2024 Jun 13;16(6):e62316. doi: 10.7759/cureus.62316. eCollection 2024 Jun. Cureus. 2024. PMID: 39006625 Free PMC article. Review.
-
Treatment Tolerability in Patients with Immunoglobulin Light-Chain Amyloidosis.Am Health Drug Benefits. 2018 Nov;11(8):430-437. Am Health Drug Benefits. 2018. PMID: 30647830 Free PMC article.
-
Auto-SCT improves survival in systemic light chain amyloidosis: a retrospective analysis with 14-year follow-up.Bone Marrow Transplant. 2014 Aug;49(8):1036-41. doi: 10.1038/bmt.2014.115. Epub 2014 Jun 2. Bone Marrow Transplant. 2014. PMID: 24887378 Clinical Trial.
-
Progress and challenges in the treatment of cardiac amyloidosis: a review of the literature.ESC Heart Fail. 2021 Aug;8(4):2380-2396. doi: 10.1002/ehf2.13443. Epub 2021 Jun 5. ESC Heart Fail. 2021. PMID: 34089308 Free PMC article. Review.
-
Light chain amyloidosis: the heart of the problem.Haematologica. 2013 Oct;98(10):1492-5. doi: 10.3324/haematol.2013.094482. Haematologica. 2013. PMID: 24091927 Free PMC article. No abstract available.
References
-
- Gertz MA. Immunoglobulin light chain amyloidosis: 2011 update on diagnosis, risk-stratification, and management. Am J Hematol. 2011;86(2):180–186. - PubMed
-
- Merlini G, Palladini G. Amyloidosis: is a cure possible? Ann Oncol. 2008;19(Suppl 4):iv63–66. - PubMed
-
- Skinner M. AL amyloidosis: the last 30 years. Amyloid. 2000;7(1):13–14. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
