

Effects of motion, attenuation, and scatter corrections on gated cardiac SPECT reconstruction
- PMID: 22149839
- PMCID: PMC3247926
- DOI: 10.1118/1.3660328
Effects of motion, attenuation, and scatter corrections on gated cardiac SPECT reconstruction
Abstract
Purpose: In gated cardiac single photon emission computed tomography (SPECT), image reconstruction is often hampered by various degrading factors including depth-dependent spatial blurring, attenuation, scatter, motion blurring, and low data counts. Consequently, there has been significant development in image reconstruction methods for improving the quality of reconstructed images. The goal of this work is to investigate how these degrading factors will impact the reconstructed myocardium when different reconstruction methods are used.
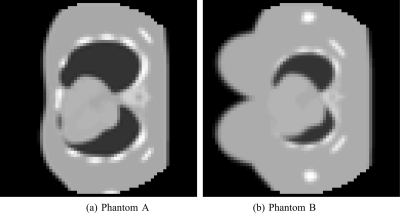
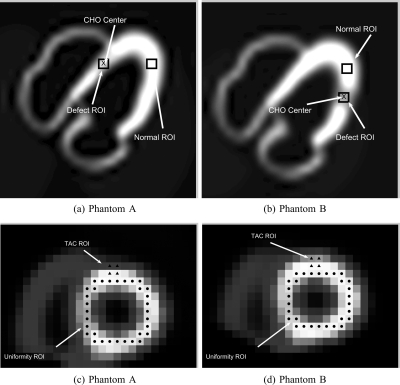
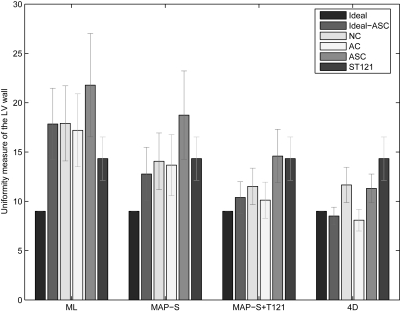
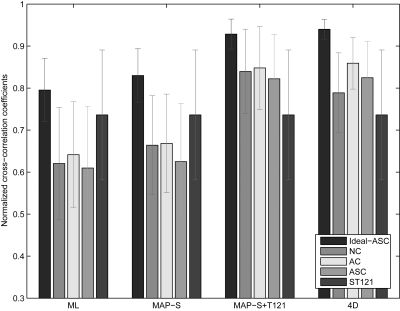
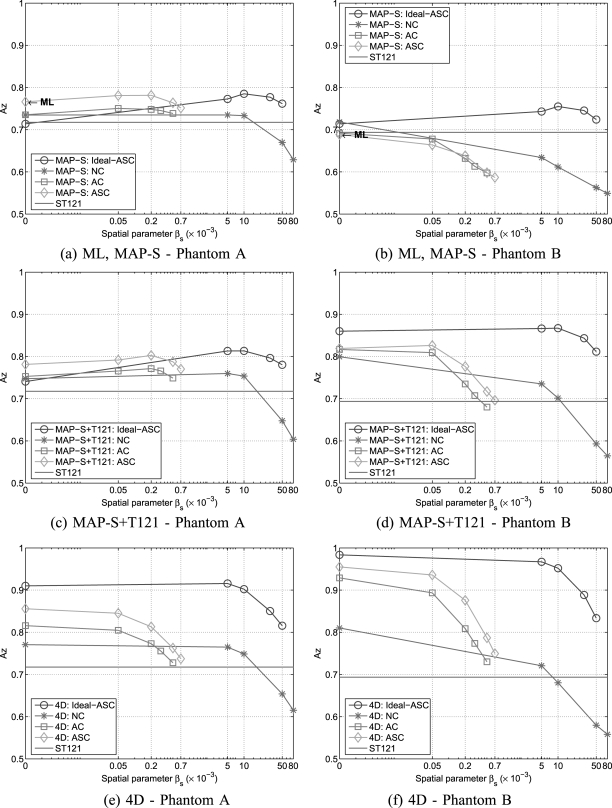
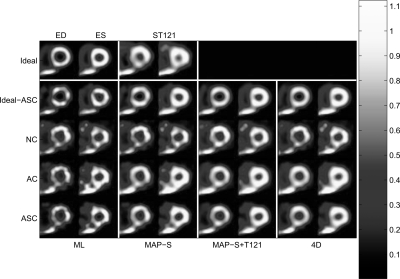
Methods: The authors conduct a comparative study of the effects of these degrading factors on the accuracy of myocardium by several reconstruction algorithms, including (1) a clinical spatiotemporal processing method, (2) maximum likelihood (ML) estimation, (3) 3D maximum a posteriori (MAP) estimation, (4) 3D MAP with posttemporal filtering, and (5) motion-compensated spatiotemporal (4D) reconstruction. To quantify the reconstruction results, the authors use the following measures on different aspects of the myocardium: (1) overall error level in the myocardium, (2) regional accuracy of the left ventricle (LV) wall, (3) uniformity of the LV, (4) accuracy of regional time activity curves by normalized cross-correlation coefficient, and (5) perfusion defect detectability. The authors also assess the effectiveness of degrading corrections in reconstruction by considering an upper bound for each reconstruction method, which represents what would be achieved by each method if the acquired data were free from attenuation and scatter degradations. In the experiments the authors use Monte Carlo simulated cardiac gated SPECT imaging based on the 4D NURBS-based cardiac-torso (NCAT) phantom with different patient geometry and lesion settings, in which the simulated ground truth is known for the purpose of quantitative evaluation.
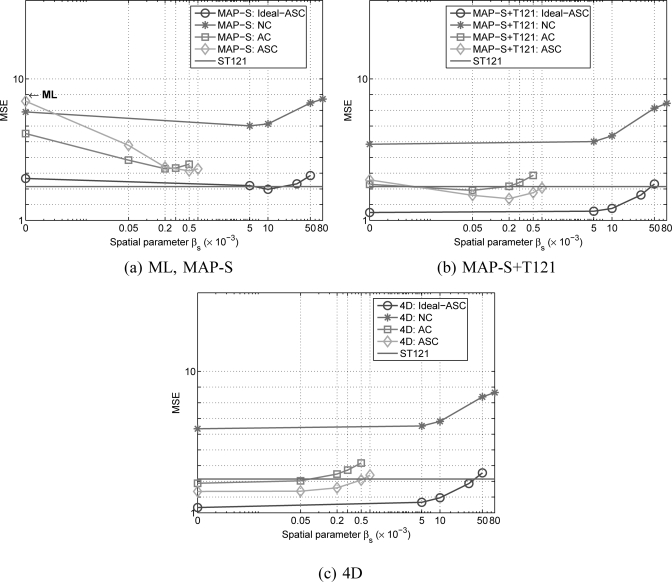
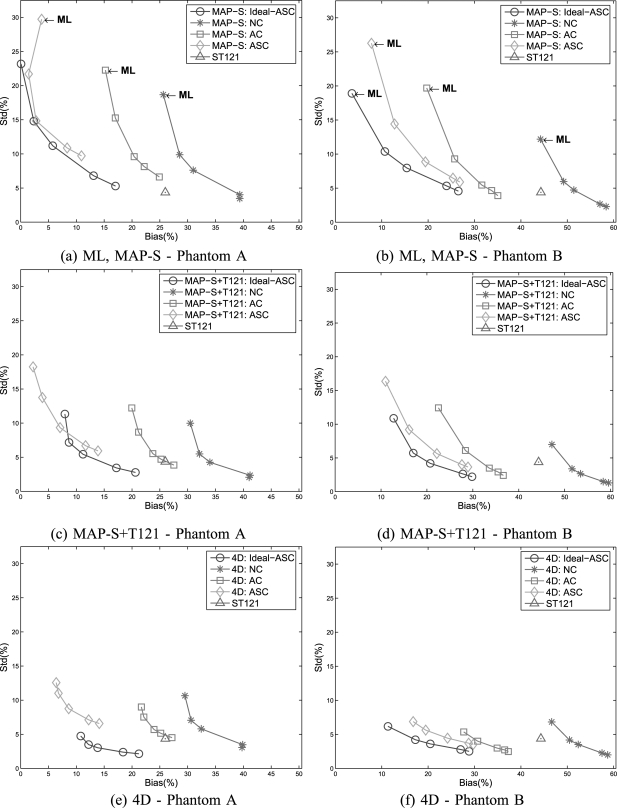
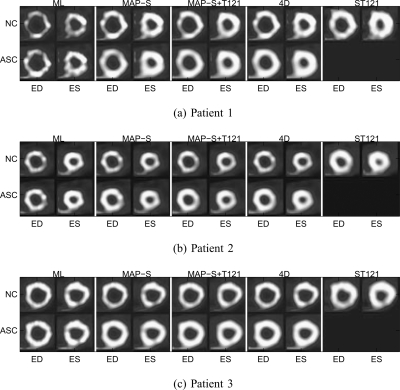
Results: The results demonstrate that use of temporal processing in reconstruction (Methods 1, 4, and 5 above) can greatly improve the reconstructed myocardium in terms of both error level and perfusion defect detection. In low-count gated studies, it can have even greater impact than other degrading factors. Both attenuation and scatter corrections can lead to reduced error levels in the myocardium in all methods; in particular, with 4D the bias can be reduced by as much as four-fold compared to no correction. There is a slight increase in noise level observed with scatter correction. A significant improvement in heart wall appearance is demonstrated in reconstruction results from three sets of clinical acquisitions as correction for degradations is combined with refinement of temporal filtering.
Conclusions: Correction for degrading factors such as resolution, attenuation, scatter, and motion blur can all lead to improved image quality in cardiac gated SPECT reconstruction. However, their effectiveness could also vary with the reconstruction algorithms used. Both attenuation and scatter corrections can effectively reduce the bias level of the reconstructed LV wall, though scatter correction is also observed to increase the variance level. Use of temporal processing in reconstruction can have greater impact on the accuracy of the myocardium than correction of other degrading factors. Overall, use of degrading corrections in 4D reconstruction is shown to be most effective for improving both reconstruction accuracy of the myocardium and detectability of perfusion defects in gated images.
Figures
Similar articles
-
A quantitative evaluation study of four-dimensional gated cardiac SPECT reconstruction.Phys Med Biol. 2009 Sep 21;54(18):5643-59. doi: 10.1088/0031-9155/54/18/019. Epub 2009 Sep 1. Phys Med Biol. 2009. PMID: 19724094 Free PMC article.
-
A quantitative study of motion estimation methods on 4D cardiac gated SPECT reconstruction.Med Phys. 2012 Aug;39(8):5182-93. doi: 10.1118/1.4738377. Med Phys. 2012. PMID: 22894443 Free PMC article.
-
4D reconstruction for low-dose cardiac gated SPECT.Med Phys. 2013 Feb;40(2):022501. doi: 10.1118/1.4773868. Med Phys. 2013. PMID: 23387768 Free PMC article.
-
Artificial Intelligence-Based Data Corrections for Attenuation and Scatter in Position Emission Tomography and Single-Photon Emission Computed Tomography.PET Clin. 2021 Oct;16(4):543-552. doi: 10.1016/j.cpet.2021.06.010. Epub 2021 Aug 5. PET Clin. 2021. PMID: 34364816 Free PMC article. Review.
-
PET/CT Image Artifacts Caused by the Arms.J Nucl Med Technol. 2021 Mar;49(1):19-22. doi: 10.2967/jnmt.120.248641. Epub 2020 Jul 24. J Nucl Med Technol. 2021. PMID: 32709674 Review.
Cited by
-
Variation of Contrast Values for Myocardial Perfusion Imaging in Single-photon Emission Computed Tomography/Computed Tomography Hybrid Systems with Different Correction Methods.J Clin Imaging Sci. 2020 Sep 25;10:58. doi: 10.25259/JCIS_123_2020. eCollection 2020. J Clin Imaging Sci. 2020. PMID: 33024613 Free PMC article.
-
Motion-compensated image reconstruction vs postreconstruction correction in respiratory-binned SPECT with standard and reduced-dose acquisitions.Med Phys. 2018 Jul;45(7):2991-3000. doi: 10.1002/mp.12932. Epub 2018 May 13. Med Phys. 2018. PMID: 29679508 Free PMC article.
-
Limited-angle effect compensation for respiratory binned cardiac SPECT.Med Phys. 2016 Jan;43(1):443. doi: 10.1118/1.4938579. Med Phys. 2016. PMID: 26745937 Free PMC article.
-
4D non-local means post-filtering for cardiac gated SPECT.Phys Med Biol. 2018 Jan 31;63(3):035026. doi: 10.1088/1361-6560/aaa44d. Phys Med Biol. 2018. PMID: 29283356 Free PMC article.
-
4-D Reconstruction With Respiratory Correction for Gated Myocardial Perfusion SPECT.IEEE Trans Med Imaging. 2017 Aug;36(8):1626-1635. doi: 10.1109/TMI.2017.2690819. Epub 2017 Apr 4. IEEE Trans Med Imaging. 2017. PMID: 28391190 Free PMC article.
References
-
- Gilland D. R., Mair B. A., Bowsher J. E., and Jaszczak R. J., “Simultaneous reconstruction and motion estimation for gated cardiac ECT,” IEEE Trans. Nucl. Sci. 49, pp. 2344–2349 (2002).10.1109/TNS.2002.803820 - DOI
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
