

'Extreme' vasculobiliary injuries: association with fundus-down cholecystectomy in severely inflamed gallbladders
- PMID: 22151444
- PMCID: PMC3252984
- DOI: 10.1111/j.1477-2574.2011.00393.x
'Extreme' vasculobiliary injuries: association with fundus-down cholecystectomy in severely inflamed gallbladders
Abstract
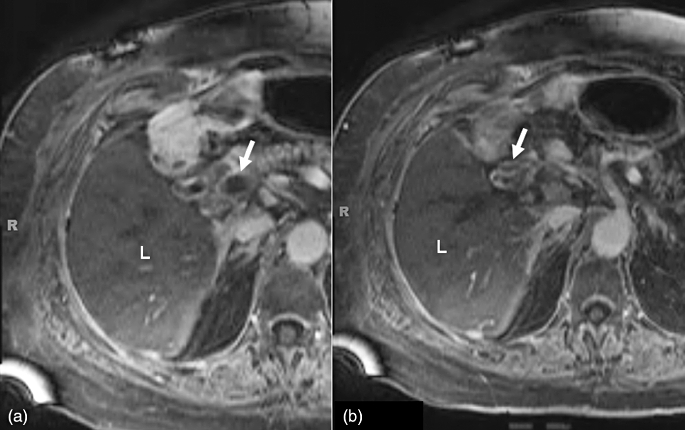
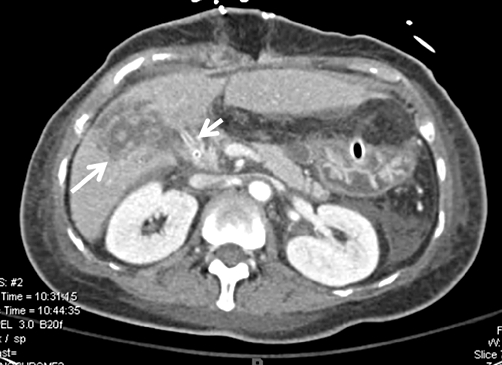
Objectives: Extreme vasculobiliary injuries usually involve major hepatic arteries and portal veins. They are rare, but have severe consequences, including rapid infarction of the liver. The pathogenesis of these injuries is not well understood. The purpose of this study was to elucidate the mechanism of injury through an analysis of clinical records, particularly the operative notes of the index procedure.
Methods: Biliary injury databases in two institutions were searched for data on extreme vasculobiliary injuries. Operative notes for the index procedure (cholecystectomy) were requested from the primary institutions. These notes and the treatment records of the tertiary centres to which the patients had been referred were examined. Radiographs from the primary institutions, when available, as well as those from the tertiary centres, were studied.
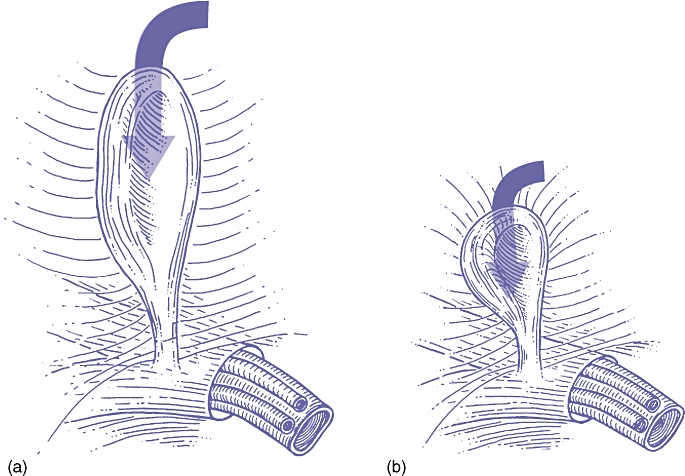
Results: Eight patients with extreme vasculobiliary injuries were found. Most had the following features in common. The operation had been started laparoscopically and converted to an open procedure because of severe chronic or acute inflammation. Fundus-down cholecystectomy had been attempted. Severe bleeding had been encountered as a result of injury to a major portal vein and hepatic artery. Four patients have required right hepatectomy and one had required an orthotopic liver transplant. Four of the eight patients have died and one remains under treatment.
Conclusions: Extreme vasculobiliary injuries tend to occur when fundus-down cholecystectomy is performed in the presence of severe inflammation. Contractive inflammation thickens and shortens the cystic plate, making separation of the gallbladder from the liver hazardous.
© 2011 International Hepato-Pancreato-Biliary Association.
Figures


References
-
- Stewart L, Robinson TN, Lee CM, Liu K, Whang K, Way LW. Right hepatic artery injury associated with laparoscopic bile duct injury: incidence, mechanism, and consequences. J Gastrointest Surg. 2004;8:523–530. - PubMed
-
- Felekouras E, Megas T, Michail OP, Papaconstantinou I, Nikiteas N, Dimitroulis D, et al. Emergency liver resection for combined biliary and vascular injury following laparoscopic cholecystectomy: case report and review of the literature. South Med J. 2007;100:317–320. - PubMed
-
- Frilling A, Li J, Weber F, Fruhauf NR, Engel J, Beckebaum S, et al. Major bile duct injuries after laparoscopic cholecystectomy: a tertiary centre experience. J Gastrointest Surg. 2004;8:679–685. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
