

Vascular architecture in anomalous right-sided ligamentum teres: three-dimensional analyses in 35 patients
- PMID: 22151449
- PMCID: PMC3252989
- DOI: 10.1111/j.1477-2574.2011.00398.x
Vascular architecture in anomalous right-sided ligamentum teres: three-dimensional analyses in 35 patients
Abstract
Background: Right-sided ligamentum teres (RSLT) is a congenital anomaly that is sometimes encountered during hepatobiliary surgeries. However, a valid protocol for describing the segmental anatomy of livers with RSLT has not been established, and confusions or anatomic misunderstandings have been a major problem.
Methods: The vascular architecture and morphological characteristics were investigated in 35 livers with RSLT using three-dimensional (3D) simulations.
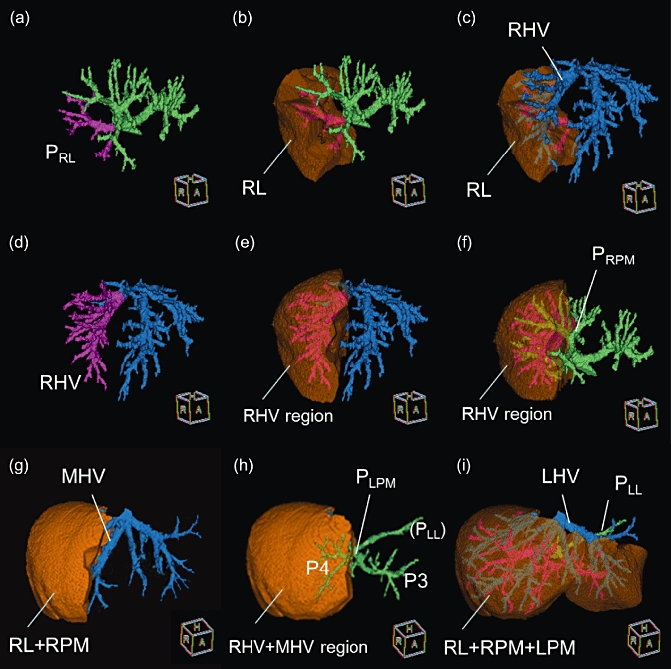
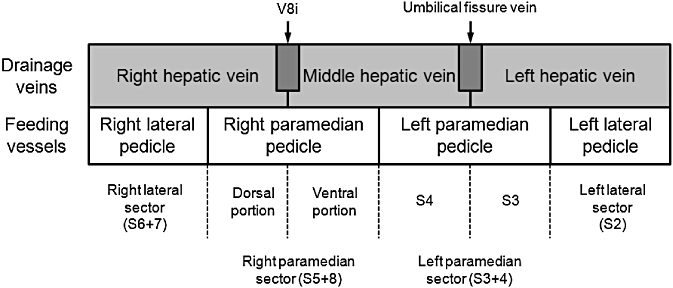
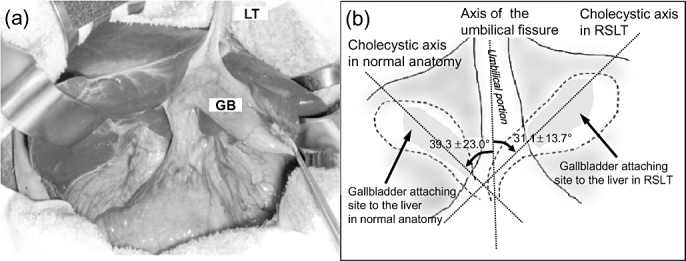
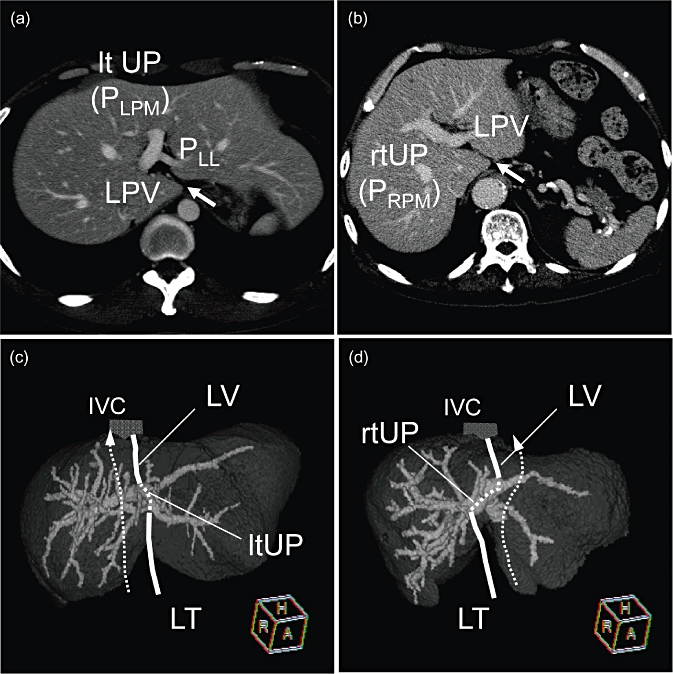
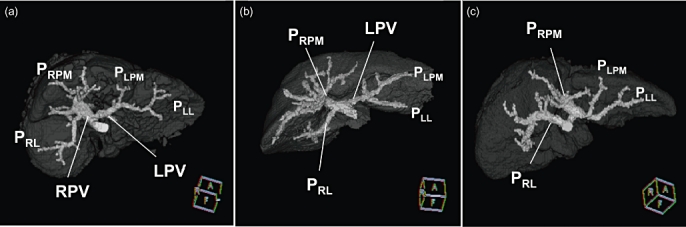
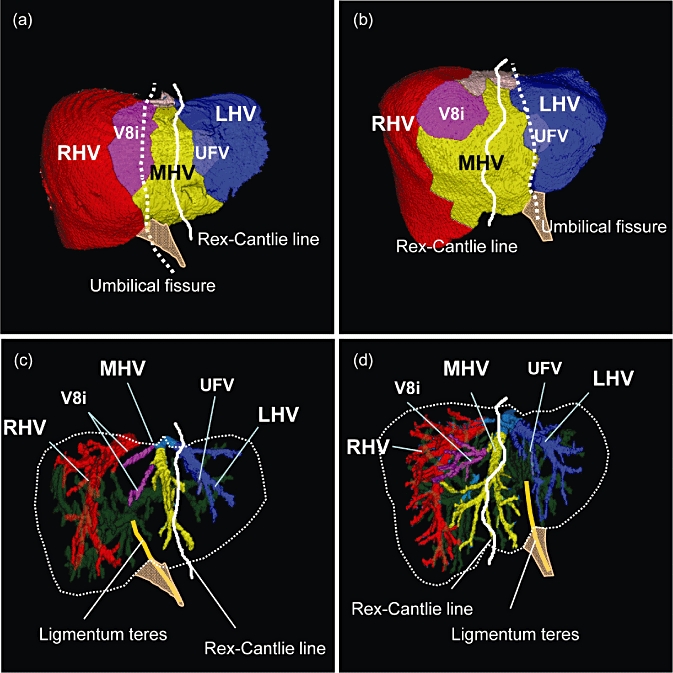
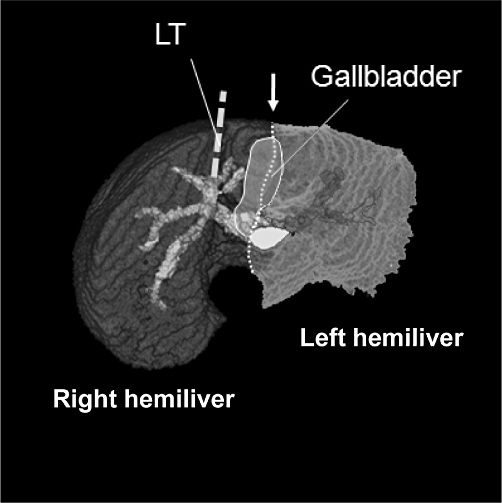
Results: Couinaud's four sectors and three hepatic veins were clearly distinguished in the liver with RSLT using 3D simulations. The ligamentum teres was connected with the right paramedian portal pedicle, and the long axis of the cystic fossa was always observed on the left of the ligamentum teres in all 35 livers. However, when the main portal scissura was visualized using 3D simulation, the gallbladder was always located on the border of either side of the hemilivers, and the malposition of the gallbladder was not confirmed.
Conclusions: Although the right-sided components of the livers are well developed as a result of the right-dominant distribution of the feeding vessels in livers with RSLT, the basic segmental structure defined by the four sectors and the three hepatic veins are as well preserved as those in the typical liver anatomy.
© 2011 International Hepato-Pancreato-Biliary Association.
Figures
References
-
- Maetani Y, Itoh K, Kojima N, Tabuchi T, Shibata T, Asonuma K, et al. Portal vein anomaly associated with deviation of the ligamentum teres to the right and malposition of the gallbladder. Radiology. 1998;207:723–728. - PubMed
-
- Uesaka K, Yasui K, Morimoto T, Torii A, Kodera Y, Hirai T, et al. Left-sided gallbladder with intrahepatic portal venous anomalies. J Hepatobiliary Pancreat Surg. 1995;2:425–430.
-
- Lucidarme O, Taboury J, Savier E, Cadi M, Hannoun L, Grenier PA. Fusion of the midplane with the left intersectional plane: a liver anatomical variation revisited with multidetector-row CT. Eur Radiol. 2006;16:1699–1708. - PubMed
-
- Rocca JP, Rodriguez-Davalos MI, Burke-Davis M, Marvin MR, Sheiner PA, Facciuto ME. Living-donor hepatectomy in right-sided round-ligament liver: importance of mapping the anatomy to the left medial segment. J Hepatobiliary Pancreat Surg. 2006;13:454–457. - PubMed
