

Type 1 autoimmune pancreatitis
- PMID: 22151922
- PMCID: PMC3261813
- DOI: 10.1186/1750-1172-6-82
Type 1 autoimmune pancreatitis
Abstract
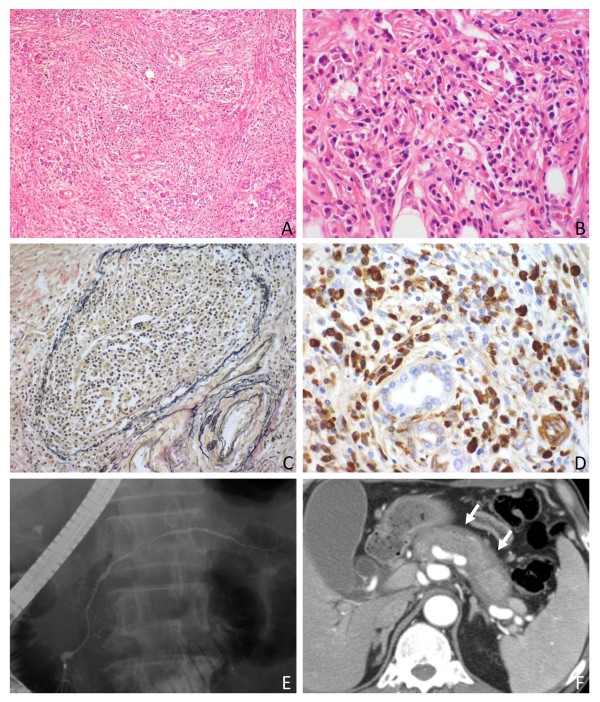
Before the concept of autoimmune pancreatitis (AIP) was established, this form of pancreatitis had been recognized as lymphoplasmacytic sclerosing pancreatitis or non-alcoholic duct destructive chronic pancreatitis based on unique histological features. With the discovery in 2001 that serum IgG4 concentrations are specifically elevated in AIP patients, this emerging entity has been more widely accepted. Classical cases of AIP are now called type 1 as another distinct subtype (type 2 AIP) has been identified. Type 1 AIP, which accounts for 2% of chronic pancreatitis cases, predominantly affects adult males. Patients usually present with obstructive jaundice due to enlargement of the pancreatic head or thickening of the lower bile duct wall. Pancreatic cancer is the leading differential diagnosis for which serological, imaging, and histological examinations need to be considered. Serologically, an elevated level of IgG4 is the most sensitive and specific finding. Imaging features include irregular narrowing of the pancreatic duct, diffuse or focal enlargement of the pancreas, a peri-pancreatic capsule-like rim, and enhancement at the late phase of contrast-enhanced images. Biopsy or surgical specimens show diffuse lymphoplasmacytic infiltration containing many IgG4+ plasma cells, storiform fibrosis, and obliterative phlebitis. A dramatic response to steroid therapy is another characteristic, and serological or radiological effects are normally identified within the first 2 or 3 weeks. Type 1 AIP is estimated as a pancreatic manifestation of systemic IgG4-related disease based on the fact that synchronous or metachronous lesions can develop in multiple organs (e.g. bile duct, salivary/lacrimal glands, retroperitoneum, artery, lung, and kidney) and those lesions are histologically identical irrespective of the organ of origin. Several potential autoantigens have been identified so far. A Th2-dominant immune reaction and the activation of regulatory T-cells are assumed to be involved in the underlying immune reaction. IgG4 antibodies have two unique biological functions, Fab-arm exchange and a rheumatoid factor-like activity, both of which may play immune-defensive roles. However, the exact role of IgG4 in this disease still remains to be clarified. It seems important to recognize this unique entity given that the disease is treatable with steroids.
Figures
Similar articles
-
Strategy to differentiate autoimmune pancreatitis from pancreas cancer.World J Gastroenterol. 2012 Mar 14;18(10):1015-20. doi: 10.3748/wjg.v18.i10.1015. World J Gastroenterol. 2012. PMID: 22416175 Free PMC article. Review.
-
Autoimmune pancreatitis and IgG4-related sclerosing cholangitis.Curr Opin Rheumatol. 2011 Jan;23(1):80-7. doi: 10.1097/BOR.0b013e3283412f60. Curr Opin Rheumatol. 2011. PMID: 21124090 Review.
-
Autoimmune pancreatitis: proposal of IgG4-related sclerosing disease.J Gastroenterol. 2006 Jul;41(7):613-25. doi: 10.1007/s00535-006-1862-6. J Gastroenterol. 2006. PMID: 16932997 Free PMC article. Review.
-
Autoimmune pancreatitis and IgG4-related sclerosing disease.Nat Rev Gastroenterol Hepatol. 2010 Jul;7(7):401-9. doi: 10.1038/nrgastro.2010.81. Epub 2010 Jun 15. Nat Rev Gastroenterol Hepatol. 2010. PMID: 20548323 Review.
-
Autoimmune pancreatitis: an underdiagnosed autoimmune disease with clinical, imaging and serological features.Autoimmun Rev. 2010 Feb;9(4):237-40. doi: 10.1016/j.autrev.2009.07.003. Epub 2009 Jul 18. Autoimmun Rev. 2010. PMID: 19622398 Review.
Cited by
-
IgG4-related renal disease: clinical and pathological characteristics.Int J Clin Exp Pathol. 2014 Aug 15;7(9):6379-85. eCollection 2014. Int J Clin Exp Pathol. 2014. PMID: 25337295 Free PMC article. Review.
-
Autoimmune pancreatitis can develop into chronic pancreatitis.Orphanet J Rare Dis. 2014 May 21;9:77. doi: 10.1186/1750-1172-9-77. Orphanet J Rare Dis. 2014. PMID: 24884922 Free PMC article.
-
Type 1 autoimmune pancreatitis can transform into chronic pancreatitis: a long-term follow-up study of 73 Japanese patients.Int J Rheumatol. 2013;2013:272595. doi: 10.1155/2013/272595. Epub 2013 May 16. Int J Rheumatol. 2013. PMID: 23762066 Free PMC article.
-
Extracorporeal shock wave lithotripsy treatment of pancreatic stones complicated with advanced stage autoimmune pancreatitis.BMC Gastroenterol. 2015 Mar 10;15:28. doi: 10.1186/s12876-015-0255-9. BMC Gastroenterol. 2015. PMID: 25887404 Free PMC article.
-
IgG4-related sclerosing cholangitis: all we need to know.J Gastroenterol. 2016 Apr;51(4):295-312. doi: 10.1007/s00535-016-1163-7. Epub 2016 Jan 27. J Gastroenterol. 2016. PMID: 26817943 Review.
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
