

Baseline characteristics and hospital mortality in the Acute Heart Failure Database (AHEAD) Main registry
- PMID: 22152228
- PMCID: PMC3388663
- DOI: 10.1186/cc10584
Baseline characteristics and hospital mortality in the Acute Heart Failure Database (AHEAD) Main registry
Abstract
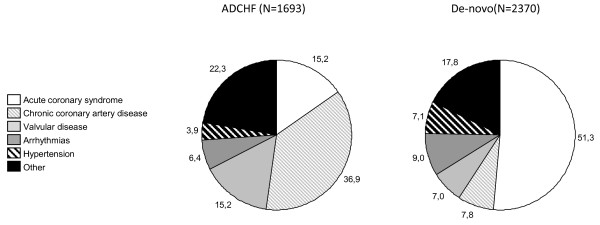
Introduction: The prognosis of patients hospitalized with acute heart failure (AHF) is poor and risk stratification may help clinicians guide care. The objectives of the Acute Heart Failure Database (AHEAD) registry are to assess patient characteristics, etiology, treatment and outcome of AHF.
Methods: The AHEAD main registry includes patients hospitalized for AHF in seven centers with a Catheterization Laboratory Service in the Czech Republic. The data were collected from September 2006 to October 2009. The inclusion criteria for the database adhere to the European guidelines for AHF (2005) and patients were systematically classified according to the basic syndromes, type and etiology of AHF.
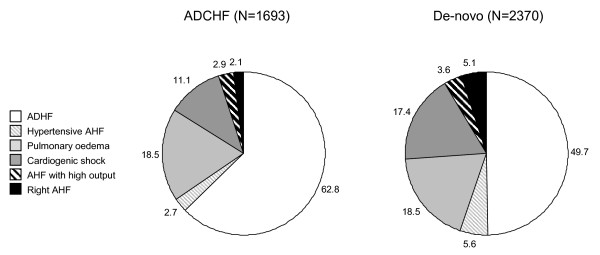
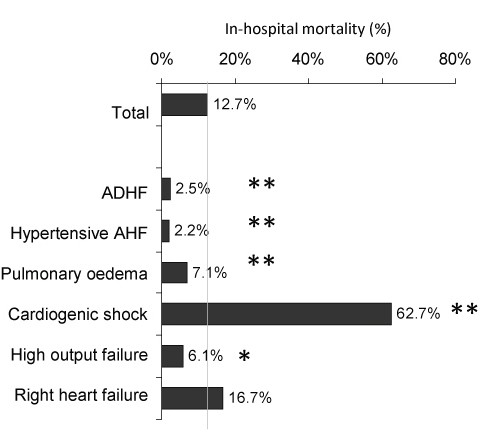
Results: Of 4,153 patients, 12.7% died during hospitalization. The median length of hospitalization was 7.1 days. Mean age of patients was 71.5 ± 12.4 years; men were younger (68.6 ± 12.4 years) compared to women (75.5 ± 11.5 years) (P < 0.001). De-novo heart failure was seen in 58.3% of the patients. According to the classification of heart failure syndromes, acute decompensated heart failure (ADHF) was reported in 55.3%, hypertensive AHF in 4.4%, pulmonary edema in 18.4%, cardiogenic shock in 14.7%, high output failure in 3.3%, and right heart failure in 3.8%. The mortality of cardiogenic shock was 62.7%, of right AHF 16.7%, of pulmonary edema 7.1%, of high output HF 6.1%, whereas the mortality of hypertensive AHF or ADHF was < 2.5%. According to multivariate analyses, low systolic blood pressure, low cholesterol level, hyponatremia, hyperkalemia, the use of inotropic agents and norepinephrine were predictive parameters for in-hospital mortality in patients without cardiogenic shock. Severe left ventricular dysfunction and renal insufficiency were predictive parameters for mortality in patients with cardiogenic shock. Invasive ventilation and age over 70 years were the most important predictive factors for mortality in both genders with or without cardiogenic shock.
Conclusions: The AHEAD Main registry provides up-to-date information on the etiology, treatment and hospital outcomes of patients hospitalized with AHF. The results highlight the highest risk patients.
Figures
References
-
- Nieminen MS, Brutsaert D, Dickstein K, Drexler H, Follath F, Harjola VP, Hochadel M, Komajda M, Lassus J, Lopez-Sendon JL, Ponikowski P, Tavazzi L. EuroHeart Survey Investigators; Heart Failure Association; European Society of Cardiology. EuroHeart Failure Survey II (EHFS II): a survey on hospitalized acute heart failure patients: description of population. Eur Heart J. 2006;27:2725–2736. doi: 10.1093/eurheartj/ehl193. - DOI - PubMed
-
- Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, Ferguson TB, Ford E, Furie K, Gillespie C, Go A, Greenlund K, Haase N, Hailpern S, Ho PM, Howard V, Kissela B, Kittner S, Lackland D, Lisabeth L, Marelli A, McDermott MM, Meigs J, Mozaffarian D, Mussolino M, Nichol G, Roger VL, Rosamond W, Sacco R, Sorlie P, Stafford R, Thom T, Wasserthiel-Smoller S, Wong ND, Wylie-Rosett J. American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Executive Summary: Heart Disease and Stroke Statistics--2010 Update: a report from the American Heart Association. Circulation. 2010;121:948–954. - PubMed
-
- Nieminen MS, Böhm M, Cowie MR, Drexler H, Filippatos GS, Jondeau G, Hasin Y, Lopez-Sendon J, Mebazaa A, Metra M, Rhodes A, Swedberg K, Priori SG, Garcia MA, Blanc JJ, Budaj A, Cowie MR, Dean V, Deckers J, Burgos EF, Lekakis J, Lindahl B, Mazzotta G, Morais J, Oto A, Smiseth OA, Garcia MA, Dickstein K, Albuquerque A, Conthe P, Crespo-Leiro M, Ferrari R, Follath F, Gavazzi A, Janssens U, Komajda M, Morais J, Moreno R, Singer M, Singh S, Tendera M, Thygesen K. ESC Committe for Practice Guideline (CPG) Executive summary of the guidelines on the diagnosis and treatment of acute heart failure. Eur Heart J. 2005;26:384–416. - PubMed
-
- Adams KF, Linderfeld J, Arnold JMO. HFSA 2006 comprehensive heart failure practice guideline. J Card Fail. 2006;26:e121–e122.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
