

Acute infective conjunctivitis in primary care: who needs antibiotics? An individual patient data meta-analysis
- PMID: 22152728
- PMCID: PMC3162176
- DOI: 10.3399/bjgp11X593811
Acute infective conjunctivitis in primary care: who needs antibiotics? An individual patient data meta-analysis
Abstract
Background: Acute infective conjunctivitis is a common problem in primary care, traditionally managed with topical antibiotics. A number of clinical trials have questioned the benefit of topical antibiotics for patients with acute infective conjunctivitis.
Aim: To determine the benefit of antibiotics for the treatment of acute infective conjunctivitis in primary care and which subgroups benefit most.
Design: An individual patient data meta-analysis.
Method: Relevant trials were identified and individual patient data gathered for meta-analysis and subgroup analysis.
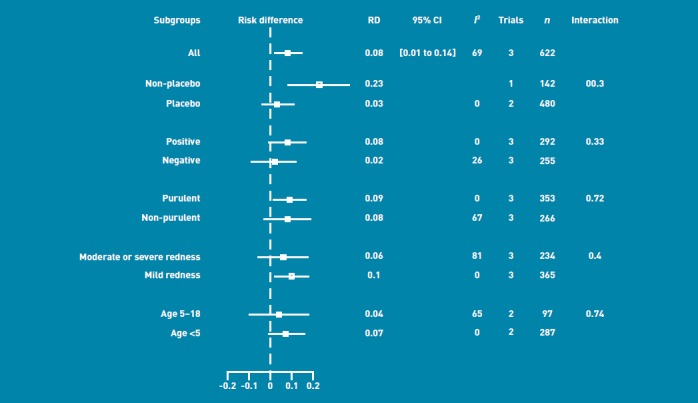
Results: Three eligible trials were identified. Individual patient data were available from all primary care trials and data were available for analysis in 622 patients. Eighty per cent (246/308) of patients who received antibiotics and 74% (233/314) of controls were cured at day 7. There was a significant benefit of antibiotics versus control for cure at seven days in all cases combined (risk difference 0.08, 95% confidence interval (CI) = 0.01 to 0.14). Subgroups that showed a significant benefit from antibiotics were patients with purulent discharge (risk difference 0.09, 95% CI = 0.01 to 0.17) and patients with mild severity of red eye (risk difference 0.10, 95% CI = 0.02 to 0.18), while the type of control used (placebo drops versus nothing) showed a statistically significant interaction (P=0.03).
Conclusion: Acute conjunctivitis seen in primary care can be thought of as a self-limiting condition, with most patients getting better regardless of antibiotic therapy. Patients with purulent discharge or a mild severity of red eye may have a small benefit from antibiotics. Prescribing practices need to be updated, taking into account these results.
Figures
Comment in
-
Prescribing safety: the case of inappropriate medicines.Br J Gen Pract. 2011 Sep;61(590):542-3. doi: 10.3399/bjgp11X593730. Br J Gen Pract. 2011. PMID: 22152727 Free PMC article. No abstract available.
-
Acute conjunctivitis in primary care: antibiotics and placebo associated with small increase in the proportion cured by 7 days compared with no treatment.Evid Based Med. 2012 Dec;17(6):177-8. doi: 10.1136/ebmed-2012-100562. Epub 2012 Apr 17. Evid Based Med. 2012. PMID: 22511644 No abstract available.
Similar articles
-
Effect of Topical Antibiotics on Duration of Acute Infective Conjunctivitis in Children: A Randomized Clinical Trial and a Systematic Review and Meta-analysis.JAMA Netw Open. 2022 Oct 3;5(10):e2234459. doi: 10.1001/jamanetworkopen.2022.34459. JAMA Netw Open. 2022. PMID: 36194412 Free PMC article.
-
A randomised controlled trial of management strategies for acute infective conjunctivitis in general practice.BMJ. 2006 Aug 12;333(7563):321. doi: 10.1136/bmj.38891.551088.7C. Epub 2006 Jul 17. BMJ. 2006. PMID: 16847013 Free PMC article. Clinical Trial.
-
[From the Cochrane Library: Marginally higher chance of cure by antibiotic treatment in acute bacterial conjunctivitis].Ned Tijdschr Geneeskd. 2007 Mar 10;151(10):594-6. Ned Tijdschr Geneeskd. 2007. PMID: 17402650 Dutch.
-
The treatment of acute infectious conjunctivitis with fusidic acid: a randomised controlled trial.Br J Gen Pract. 2005 Dec;55(521):924-30. Br J Gen Pract. 2005. PMID: 16378561 Free PMC article. Clinical Trial.
-
Chloramphenicol treatment for acute infective conjunctivitis in children in primary care: a randomised double-blind placebo-controlled trial.Lancet. 2005 Jul 2-8;366(9479):37-43. doi: 10.1016/S0140-6736(05)66709-8. Lancet. 2005. PMID: 15993231 Clinical Trial.
Cited by
-
Cancellation of the more complicated ophthalmic inpatient surgeries in a tertiary general hospital: a 10-year retrospective study.Front Med (Lausanne). 2024 Aug 29;11:1406140. doi: 10.3389/fmed.2024.1406140. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39267968 Free PMC article.
-
Infectious Disease in Contact Sports.Sports Health. 2019 Jan/Feb;11(1):47-58. doi: 10.1177/1941738118789954. Epub 2018 Aug 14. Sports Health. 2019. PMID: 30106670 Free PMC article. Review.
-
Appropriateness of Antibiotic Prescribing for Acute Conjunctivitis: A Cross-Sectional Study at a Specialist Eye Hospital in Ghana, 2021.Int J Environ Res Public Health. 2022 Sep 17;19(18):11723. doi: 10.3390/ijerph191811723. Int J Environ Res Public Health. 2022. PMID: 36141996 Free PMC article.
-
Reliability of the Evidence Addressing Treatment of Corneal Diseases: A Summary of Systematic Reviews.JAMA Ophthalmol. 2019 Jul 1;137(7):775-785. doi: 10.1001/jamaophthalmol.2019.1063. JAMA Ophthalmol. 2019. PMID: 31070698 Free PMC article.
-
Skin Microbiome Overview: How Physical Activity Influences Bacteria.Microorganisms. 2025 Apr 10;13(4):868. doi: 10.3390/microorganisms13040868. Microorganisms. 2025. PMID: 40284707 Free PMC article. Review.
References
-
- Everitt H, Little P. How do GPs diagnose and manage acute infective conjunctivitis? AGP survey. Fam Pract. 2002;19(6):658–660. - PubMed
-
- Rose P, Harnden A, Brueggemann A, et al. Chloramphenicol treatment for acute infective conjunctivitis in children in primary care: a randomised double-blind placebo-controlled trial. Lancet. 2005;366(9479):37–43. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical