

Screening for sickle cell and thalassaemia in primary care: a cost-effectiveness study
- PMID: 22152833
- PMCID: PMC3177130
- DOI: 10.3399/bjgp11X601325
Screening for sickle cell and thalassaemia in primary care: a cost-effectiveness study
Abstract
Background: Haemoglobinopathies, including sickle cell disease and thalassaemia (SCT), are inherited disorders of haemoglobin. Antenatal screening for SCT rarely occurs before 10 weeks of pregnancy.
Aim: To explore the cost-effectiveness of offering SCT screening in a primary care setting, during the pregnancy confirmation visit.
Design and setting: A model-based cost-effectiveness analysis of inner-city areas with a high proportion of residents from ethnic minority groups.
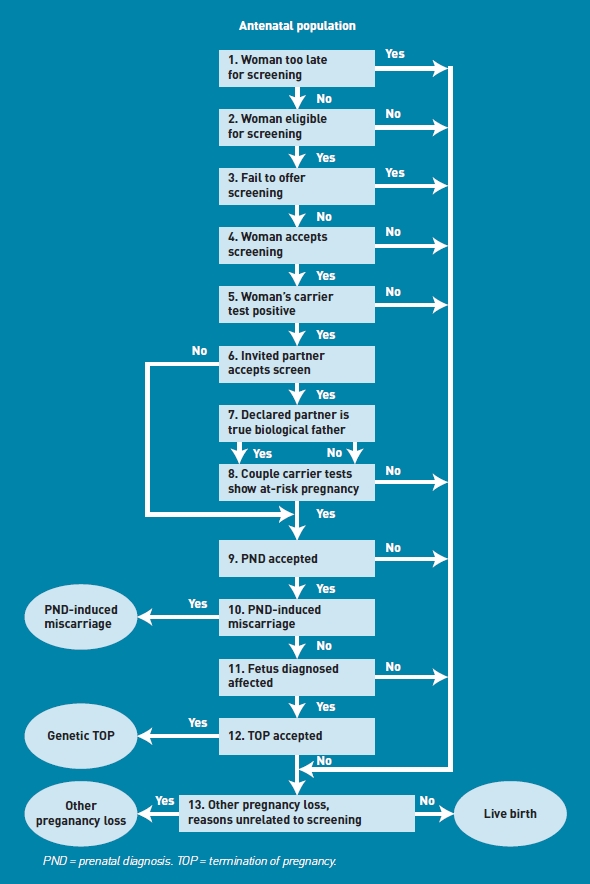
Method: Comparison was made of three SCT screening approaches: 'primary care parallel' (primary care screening with test offered to mother and father together); 'primary care sequential (primary care screening with test offered to the mother and then the father only if the mother is a carrier); and 'midwife care' (sequential screening at the first midwife consultation). The model was populated with data from the SHIFT (Screening for Haemoglobinopathies In First Trimester) trial and other sources.
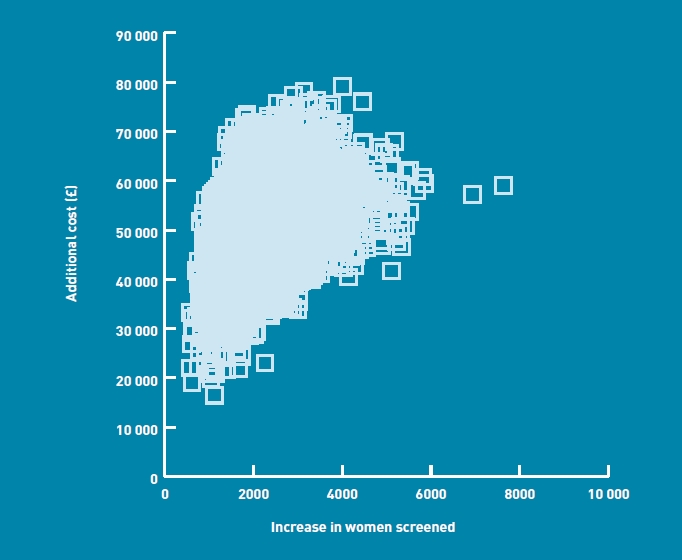
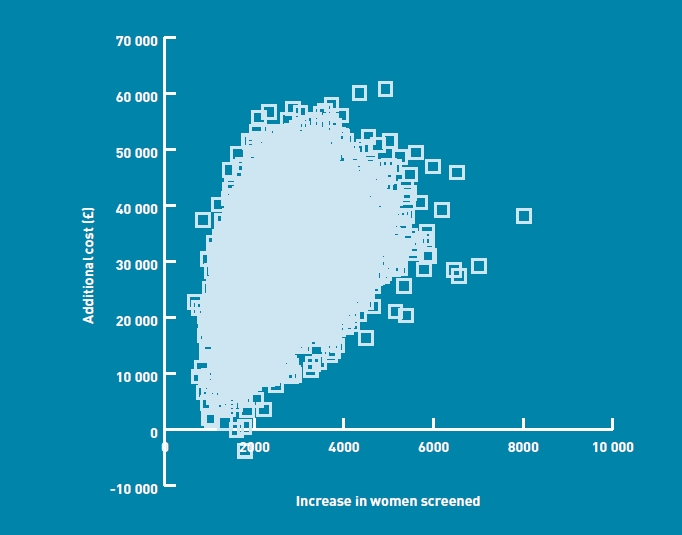
Results: Compared to midwife care, primary care sequential had a higher NHS cost of £34,000 per 10,000 pregnancies (95% confidence interval [CI] = £15,000 to £51,000) and an increase of 2623 women screened (95% CI: 1359 to 4495), giving a cost per additional woman screened by 10 weeks of £13. Primary care parallel was dominated by primary care sequential, with both higher costs and fewer women screened.
Conclusion: The policy judgement is whether an earlier opportunity for informed reproductive choice has a value of at least £13. Further work is required to understand the value attached to earlier informed reproductive choices.
Figures
Comment in
-
Commissioning maternity care: little room for manoeuvre?Br J Gen Pract. 2011 Oct;61(591):598-9. doi: 10.3399/bjgp11X601217. Br J Gen Pract. 2011. PMID: 22152824 Free PMC article. No abstract available.
-
Screening for sickle cell and thalassaemia in primary care: a cost-effectiveness study.Br J Gen Pract. 2012 Jan;62(594):13. doi: 10.3399/bjgp12X616265. Br J Gen Pract. 2012. PMID: 22520666 Free PMC article. No abstract available.
References
-
- Dormandy E, Bryan S, Gulliford M, et al. Antenatal screening for haemoglobinopathies in primary care: a cohort study and cluster randomised trial to inform a simulation model. The Screening for Haemoglobinopathies in First Trimester (SHIFT) trial. Health Technol Assess. 2010;14(20):1–160. - PubMed
-
- Zeuner D, Ades AE, Karnon J, et al. Antenatal and neonatal haemoglobinopathy screening in the UK: review and economic analysis. Health Technol Assess. 1999;3(11):i–v. 1–186. - PubMed
-
- Department of Health. NHS reference costs 2005-2006. London: Department of Health; 2006. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/Publicati... (accessed 13 Apr 2011)
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical