

Multicentric dermatofibrosarcoma protuberans in patients with adenosine deaminase-deficient severe combined immune deficiency
- PMID: 22153773
- PMCID: PMC3294021
- DOI: 10.1016/j.jaci.2011.10.028
Multicentric dermatofibrosarcoma protuberans in patients with adenosine deaminase-deficient severe combined immune deficiency
Abstract
Background: Dermatofibrosarcoma protuberans (DFSP) is a rare malignant skin tumor associated with a characteristic chromosomal translocation (t[17;22][q22;q13]) resulting in the COL1A1-platelet-derived growth factor β(PDGFB) fusion gene. This malignancy is rarely diagnosed in childhood.
Objective: We observed an unexpected high incidence of this DFSP in children affected with adenosine deaminase-deficient severe combined immunodeficiency (ADA-SCID) and set out to evaluate the association of these 2 clinical entities.
Methods: Twelve patients with ADA-SCID were evaluated with a complete dermatologic examination and skin biopsy when indicated. Conventional cytogenetic and molecular analyses (fluorescence in situ hybridization, RT-PCR, or both) were performed when possible.
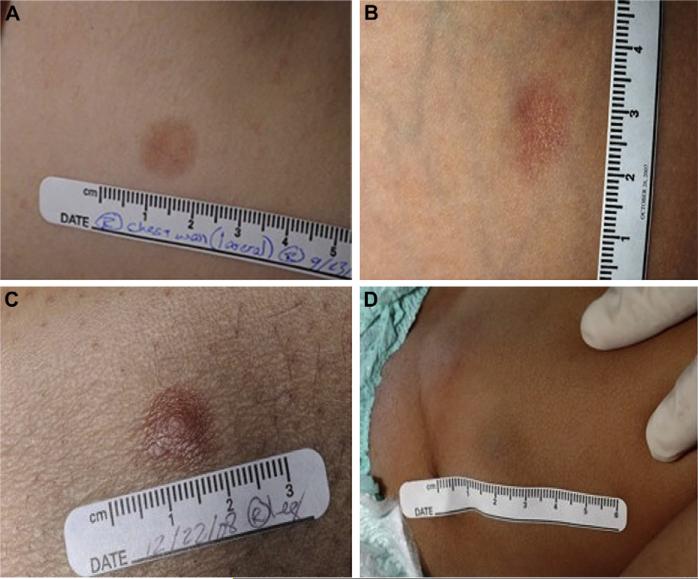
Results: Eight patients were found to have DFSP. Six patients had multicentric involvement (4-15 lesions), primarily of the trunk and extremities. Most lesions presented as 2- to 15-mm, round atrophic plaques. Nodular lesions were present in 3 patients. In all cases CD34 expression was diffusely positive, and diagnosis was confirmed either by means of cytogenetic analysis, molecular testing, or both. The characteristic DFSP-associated translocation, t(17;22)(q22;q13), was identified in 6 patients; results of fluorescence in situ hybridization were positive for fusion of the COL1A1 and PDGFB loci in 7 patients; and RT-PCR showed the COL1A1-PDGFB fusion transcript in 6 patients.
Conclusions: We describe a previously unrecognized association between ADA-SCID and DFSP with unique features, such as multicentricity and occurrence in early age. We hypothesize that the t(17;22)(q22;q13) translocation that results in dermal overexpression of PDGFB and favors the development of fibrotic tumors might arise because of the known DNA repair defect in patients with ADA-SCID. Although the natural course of DFSP in the setting of ADA-SCID is unknown, this observation should prompt regular screening for DFSP in patients with ADA-SCID.
Published by Mosby, Inc.
Figures


References
-
- Hirschorn R, Candotti F. Immunodeficiency due to defects of purine metabolism. In: Ochs H, Smith C, Puck J, editors. Primary immunodeficiency diseases. Oxford University Press; Oxford (United Kingdom): 2006. pp. 169–96.
-
- Mitchell BS, Hershfield MS. Immunodeficiency diseases caused by adenosine deaminase deficiency and purine nucleoside phosphorylase deficiency. In: Scriver CR, editor. Metabolic and molecular bases of inherited disease. 8th ed. McGraw-Hill; New York: 2001.
-
- Bowne WB, Antonescu CR, Leung DH, Katz SC, Hawkins WG, Woodruff JM, et al. Dermatofibrosarcoma protuberans: a clinicopathologic analysis of patients treated and followed at a single institution. Cancer. 2000;88:2711–20. - PubMed
-
- Fletcher CD. Pathology and genetics of tumours of soft tissue and bone (WHO classification of tumours) World Health Organization; Geneva (Switzerland):
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
