

T cell-depleted partial matched unrelated donor transplant for advanced myeloid malignancy: KIR ligand mismatch and outcome
- PMID: 22155505
- PMCID: PMC3319849
- DOI: 10.1016/j.bbmt.2011.11.024
T cell-depleted partial matched unrelated donor transplant for advanced myeloid malignancy: KIR ligand mismatch and outcome
Abstract
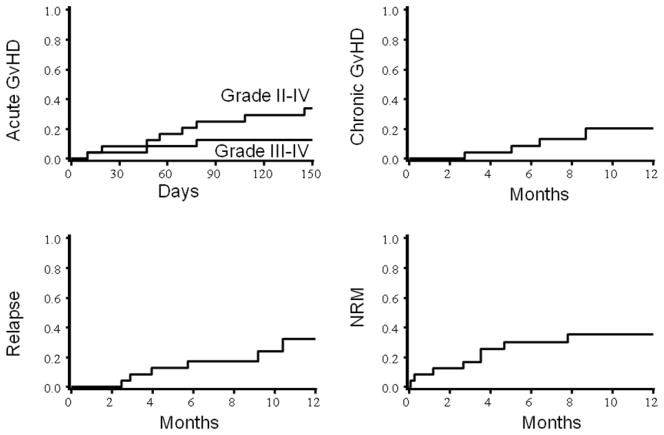
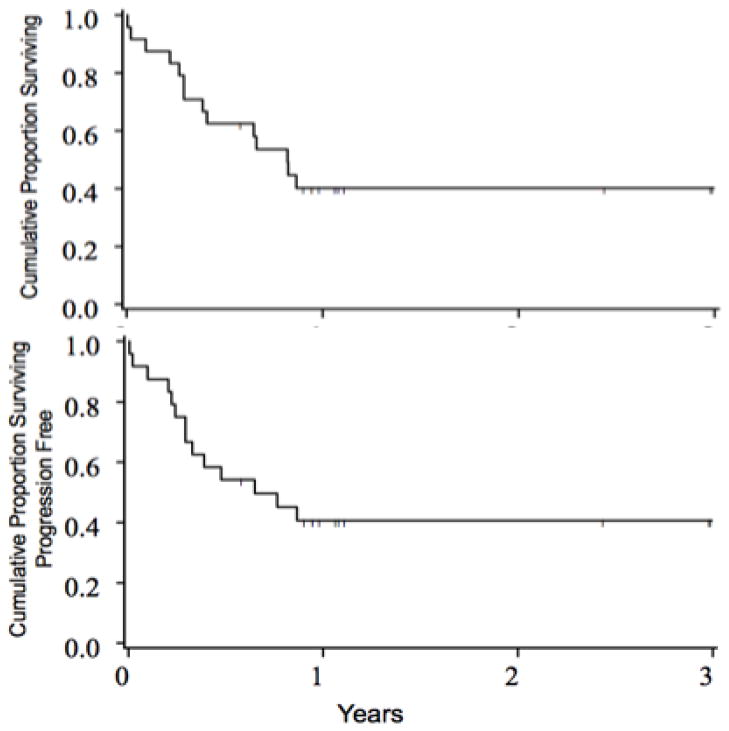
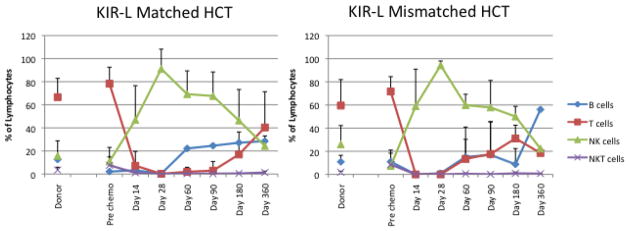
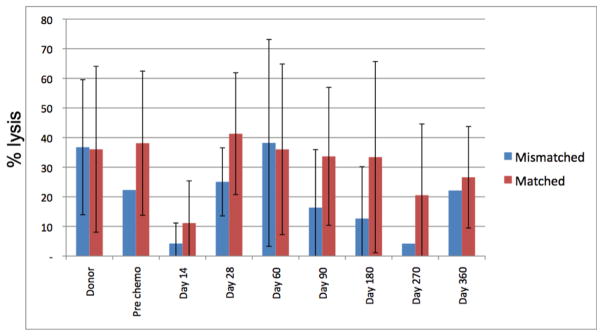
To evaluate the applicability of high-dose conditioning, CD34 selection, and enhanced natural killer (NK) cell alloreactivity reported as promising after haploidentical transplantation, we tested the same strategy for patients with advanced/high-risk myeloid leukemia lacking either related or well-matched unrelated donors (URD). In a prospective multicenter clinical trial using pretransplantation conditioning of thiotepa (5 mg/kg/day × 2), fludarabine (40 mg/mg/M(2)/day × 5), and total body radiation (800 cGy) plus thymoglobulin (2.5 mg/kg/day × 2), as well as a CD34 selected filgrastim stimulated peripheral blood graft from a partial matched URD, we treated 24 patients. The patients (median age 40 [range: 22-61]) were mismatched at 1-3 of 10 HLA loci with their donors; all were mismatched at HLA-C. Thirty-seven percent were ethnic or racial minorities. Twenty-one of 24 engrafted promptly with 1 primary graft failure and 2 early deaths. The cumulative incidence of grade II-IV acute graft-versus-host disease (aGVHD) (34%, 95% confidence interval [CI], 14-54%), chronic GVHD (20%, 95% CI, 2%-38%), and relapse (26%, 95% CI, 8%-84%) were unaffected by KIR ligand donor:recipient mismatch (n = 5) versus KIR ligand match (n = 19). Only 3 (12%) had grade III-IV GVHD. Nonrelapse occurred in 17% (95% CI, 30%-31%) by 100 days and in 35% (95% CI, 15%-55%) by 1 year. Two-year survival and leukemia-free survival were each 40% (95% CI, 21%-59%) and was similar in KIR ligand matched or mismatched patients. Infections, mostly in the first 2 months, were frequent, and were the cause of death in 5 patients (35% of deaths). T cell recovery and NK cell proliferation and functional maturation were not altered by KIR ligand match or mismatch status. For these high-risk patients, this high intensity regimen and T depleted approach yielded satisfactory outcomes, but logistical difficulties in arranging URD grafts for patients with high-risk, unstable leukemia limited accrual. Improvements in peritransplantation disease control and additional measures to augment the allogeneic graft-versus-leukemia effect are still required.
Copyright © 2012 American Society for Blood and Marrow Transplantation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Ruggeri L, Capanni M, Urbani E, et al. Effectiveness of donor natural killer cell alloreactivity in mismatched hematopoietic transplants. Science. 2002;295:2097–2100. - PubMed
-
- Aversa F, Terenzi A, Tabilio A, et al. Full haplotype-mismatched hematopoietic stem-cell transplantation: a phase II study in patients with acute leukemia at high risk of relapse. J Clin Oncol. 2005;23:3447–3454. - PubMed
-
- Giebel S, Locatelli F, Lamparelli T, et al. Survival advantage with KIR ligand incompatibility in hematopoietic stem cell transplantation from unrelated donors. Blood. 2003;102:814–819. - PubMed
-
- Davies S, Ruggeri L, DeFor T, et al. Evaluation of KIR ligand incompatibility in mismatched unrelated donor hematopoietic transplants. Blood. 2002;100:3825–3827. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
