

Karyometry in atypical endometrial hyperplasia: a Gynecologic Oncology Group study
- PMID: 22155796
- PMCID: PMC4029110
- DOI: 10.1016/j.ygyno.2011.12.422
Karyometry in atypical endometrial hyperplasia: a Gynecologic Oncology Group study
Abstract
Objectives: Treatment for atypical endometrial hyperplasia (AEH) is based on pathologic diagnosis. About 40% of AEH is found to be carcinoma at surgery. This study's objective is to derive an objective characterization of nuclei from cases diagnosed as AEH or superficially invasive endometrial cancer (SIEC).
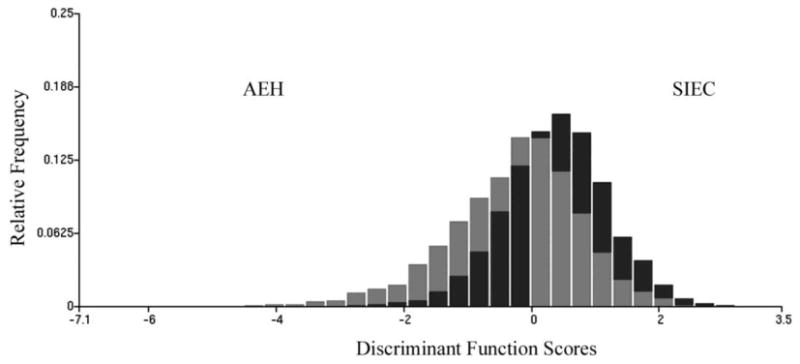
Methods: Cases from GOG study 167A were classified by a central pathology committee as AEH (n=39) or SIEC (n=39). High resolution digitized images of cell nuclei were recorded. Features of the nuclear chromatin pattern were computed. Classification rules were derived by discriminant analysis.
Results: Nuclei from cases of AEH and SIEC occupy the same range on a progression curve for endometrial lesions. Cases of AEH and SIEC both comprise nuclei of two phenotypes: hyperplastic characteristics and premalignant/neoplastic characteristics. The principal difference between AEH and SIEC is the percentage of premalignant/neoplastic nuclei. When this percentage approaches 50-60% superficial invasion is likely. SIEC may develop already from lesions at the low end of the progression curve.
Conclusions: AEH comprises cases which may constitute a low risk group involving <40% of AEH cases. These cases hold a percentage of <20% of nuclei of a preneoplastic phenotype. AEH cases from the central and high end of progression have >40% of nuclei of preneoplastic phenotype. Nuclei of the preneoplastic phenotype in AEH lesions are almost indistinguishable from nuclei in SIEC, where this percentage exceeds 60%. The percentage of nuclei of the preneoplastic phenotype in AEH esions might serve as criterion for assessment of risk for the development of invasive disease.
Copyright © 2011 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures




References
-
- Jemal AR, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58:71–96. - PubMed
-
- Parkin DM, Pisani P, Ferlay J. Estimates of the worldwide incidence of 25 major cancers in 1990. Int J Cancer. 1999;80:827–841. - PubMed
-
- Kurman RJ, Kaminski PF, Norris HJ. The behavior of endometrial hyperplasia: A long term study of “untreated” hyperplasia in 170 patients. Cancer. 1985;56:403–412. - PubMed
-
- Mazur MT. Endometrial hyperplasia/adenocarcinoma. a conventional approach. Ann Diagn Pathol. 2005;9:174–181. - PubMed
-
- Mutter GL, Zaino RJ, Baak JP, Bentley RC, Robboy SJ. Benign endometrial hyperplasia sequence and endometrial intraepithelial neoplasia. Int J Gynecol Pathol. 2007;26:103–114. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- CA 27502/CA/NCI NIH HHS/United States
- P30 CA023074/CA/NCI NIH HHS/United States
- U10 CA101165/CA/NCI NIH HHS/United States
- CA 101165/CA/NCI NIH HHS/United States
- CA 37517/CA/NCI NIH HHS/United States
- P01 CA027502/CA/NCI NIH HHS/United States
- CA 27469/CA/NCI NIH HHS/United States
- P30 CA-023074/CA/NCI NIH HHS/United States
- U10 CA027469/CA/NCI NIH HHS/United States
- CA-418190/CA/NCI NIH HHS/United States
- U10 CA037517/CA/NCI NIH HHS/United States
- K23 CA082715/CA/NCI NIH HHS/United States
- CA-82715/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
