

Association of hypo- and hyperkalemia with disease progression and mortality in males with chronic kidney disease: the role of race
- PMID: 22156587
- PMCID: PMC3267990
- DOI: 10.1159/000329511
Association of hypo- and hyperkalemia with disease progression and mortality in males with chronic kidney disease: the role of race
Abstract
Background/aims: Abnormal serum potassium is associated with higher mortality in dialysis patients, but its impact on outcomes in predialysis chronic kidney disease (CKD) is less clear. Furthermore, blacks with normal kidney function have lower urinary potassium excretion, but it is unclear if such differences have a bearing on race-associated outcomes in CKD.
Methods: We studied predialysis mortality and slopes of estimated glomerular filtration rate, eGFR) associated with serum potassium in 1,227 males with CKD. Mortality was examined in time-dependent Cox models, and slopes of eGFR in linear mixed effects models with adjustments for case mix and laboratory values.
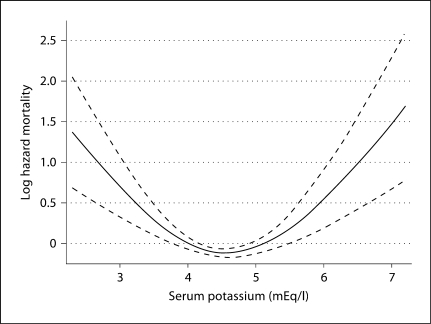
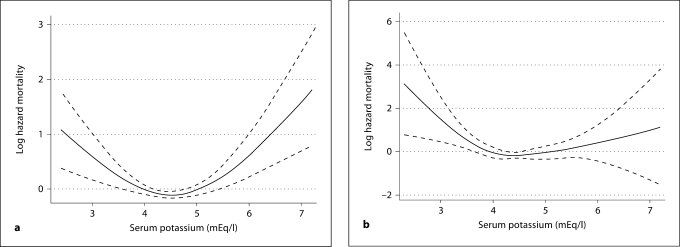
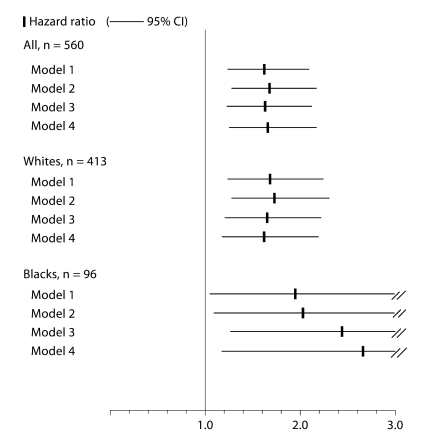
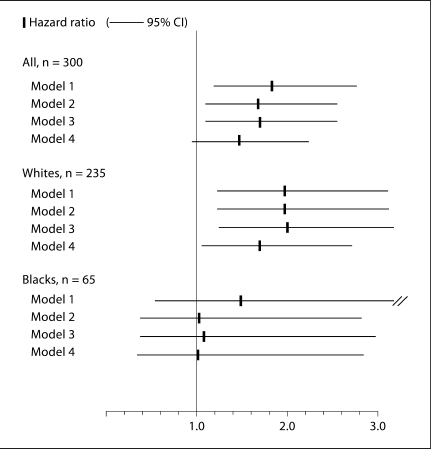
Results: Both hypo- and hyperkalemia were associated with mortality overall and in 933 white patients, but in 294 blacks hypokalemia was a stronger death predictor. Hypokalemia was associated with loss of kidney function independent of race: a 1 mEq/l lower potassium was associated with an adjusted difference in slopes of eGFR of -0.13 ml/min/1.73 m(2)/year (95% CI: -0.20 to -0.07), p < 0.001.
Conclusion: Hypo- and hyperkalemia are associated with higher mortality in CKD patients. Blacks appear to better tolerate higher potassium than whites. Hypokalemia is associated with faster CKD progression independent of race. Hyperkalemia management may warrant race-specific consideration, and hypokalemia correction may slow CKD progression.
This is a work of the US Government and is not subject to copyright protection in the USA. Foreign copyrights may apply. Published by S. Karger AG, Basel.
Figures
References
-
- Gonick HC, Kleeman CR, Rubini ME, et al. Functional impairment in chronic renal disease. Studies of potassium excretion. Am J Med Sci. 1971;261:281–290. - PubMed
-
- Lowrie EG, Lew NL. Death risk in hemodialysis patients: the predictive value of commonly measured variables and an evaluation of death rate differences between facilities. Am J Kidney Dis. 1990;15:458–482. - PubMed
-
- Iseki K, Uehara H, Nishime K, et al. Impact of the initial levels of laboratory variables on survival in chronic dialysis patients. Am J Kidney Dis. 1996;28:541–548. - PubMed
-
- Tannen RL. The influence of potassium on blood pressure. Kidney Int Suppl. 1987;22:S242–S248. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
