

Use of a rapid test of pneumococcal colonization density to diagnose pneumococcal pneumonia
- PMID: 22156852
- PMCID: PMC3275757
- DOI: 10.1093/cid/cir859
Use of a rapid test of pneumococcal colonization density to diagnose pneumococcal pneumonia
Abstract
Background: There is major need for a more sensitive assay for the diagnosis of pneumococcal community-acquired pneumonia (CAP). We hypothesized that pneumococcal nasopharyngeal (NP) proliferation may lead to microaspiration followed by pneumonia. We therefore tested a quantitative lytA real-time polymerase chain reaction (rtPCR) on NP swab samples from patients with pneumonia and controls.
Methods: In the absence of a sensitive reference standard, a composite diagnostic standard for pneumococcal pneumonia was considered positive in South African human immunodeficiency virus (HIV)-infected adults hospitalized with radiographically confirmed CAP, if blood culture, induced good-quality sputum culture, Gram stain, or urinary Binax demonstrated pneumococci. Results of quantitative lytA rtPCR in NP swab samples were compared with quantitative colony counts in patients with CAP and 300 HIV-infected asymptomatic controls.
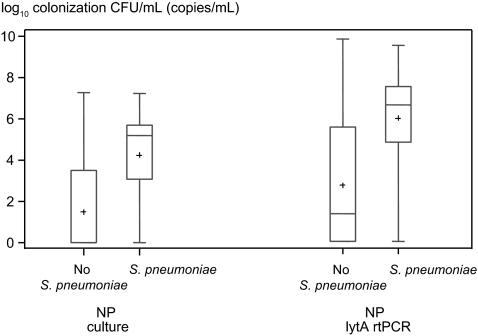
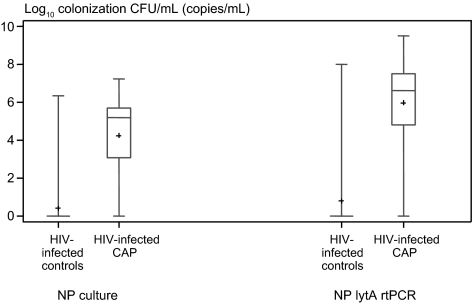
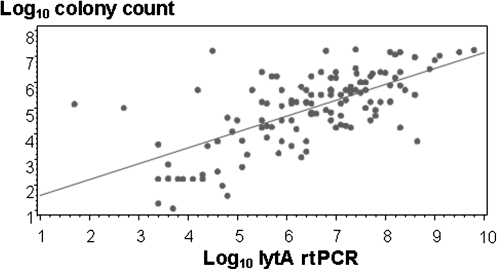
Results: Pneumococci were the leading pathogen identified in 76 of 280 patients with CAP (27.1%) using the composite diagnostic standard. NP colonization density measured by lytA rtPCR correlated with quantitative cultures (r = 0.67; P < .001). The mean lytA rtPCR copy number in patients with pneumococcal pneumonia was 6.0 log(10) copies/mL, compared with patients with CAP outside the composite standard (2.7 log(10) copies/mL; P < .001) and asymptomatic controls (0.8 log(10) copies/mL; P < .001). A lytA rtPCR density ≥8000 copies/mL had a sensitivity of 82.2% and a specificity of 92.0% for distinguishing pneumococcal CAP from asymptomatic colonization. The proportion of CAP cases attributable to pneumococcus increased from 27.1% to 52.5% using that cutoff.
Conclusions: A rapid molecular assay of NP pneumococcal density performed on an easily available specimen may significantly increase pneumococcal pneumonia diagnoses in adults.
Figures
References
-
- Scott JA, Hall AJ, Muyodi C, et al. Aetiology, outcome, and risk factors for mortality among adults with acute pneumonia in Kenya. Lancet. 2000;355:1225–30. - PubMed
-
- Bartlett JG. Decline in microbial studies for patients with pulmonary infections. Clin Infect Dis. 2004;39:170–2. - PubMed
-
- Klugman KP, Madhi SA, Albrich WC. Novel approaches to the identification of Streptococcus pneumoniae as the cause of community-acquired pneumonia. Clin Infect Dis. 2008;47(Suppl 3):S202–6. - PubMed
-
- Jokinen C, Heiskanen L, Juvonen H, et al. Microbial etiology of community-acquired pneumonia in the adult population of 4 municipalities in eastern Finland. Clin Infect Dis. 2001;32:1141–54. - PubMed
-
- Rimland D, Navin TR, Lennox JL, et al. Prospective study of etiologic agents of community-acquired pneumonia in patients with HIV infection. AIDS. 2002;16:85–95. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
