

Hospital quality and the cost of inpatient surgery in the United States
- PMID: 22156928
- PMCID: PMC3249383
- DOI: 10.1097/SLA.0b013e3182402c17
Hospital quality and the cost of inpatient surgery in the United States
Abstract
Context: Payers, policy makers, and professional organizations have launched a variety of initiatives aimed at improving hospital quality with inpatient surgery. Despite their obvious benefits for patients, the likely impact of these efforts on health care costs is uncertain. In this context, we examined relationships between hospital outcomes and expenditures in the US Medicare population.
Methods: Using the 100% national claims files, we identified all US hospitals performing coronary artery bypass graft, total hip replacement, abdominal aortic aneurysm repair, or colectomy procedures between 2005 and 2007. For each procedure, we ranked hospitals by their risk- and reliability-adjusted outcomes (complication and mortality rates, respectively) and sorted them into quintiles. We then examined relationships between hospital outcomes and risk-adjusted, 30-day episode payments.
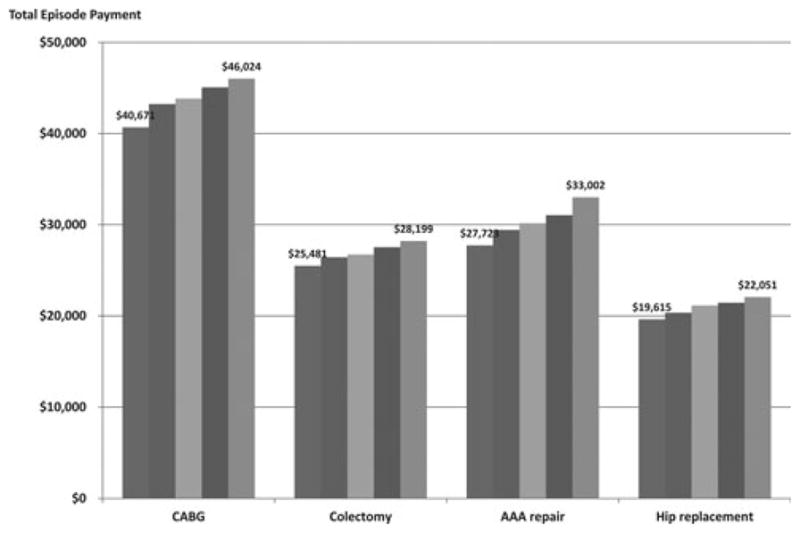
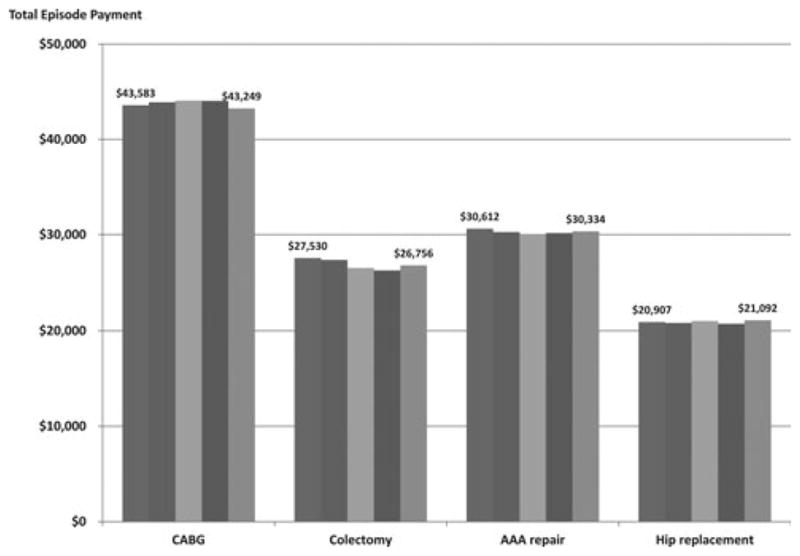
Results: There was a strong, positive correlation between hospital complication rates and episode payments for all procedures. With coronary artery bypass graft, for example, hospitals in the highest complication quintile had average payments that were $5353 per patient higher than at hospitals in the lowest quintile ($46,024 vs $40,671, P < 0.001). Payments to hospitals with high complication rates were also higher for colectomy ($2719 per patient), abdominal aortic aneurysm repair ($5279), and hip replacement ($2436). Higher episode payments at lower-quality hospitals were attributable in large part to higher payments for the index hospitalization, although 30-day readmissions, physician services, and postdischarge ancillary care also contributed. Despite the strong association between hospital complication rates and payments, hospital mortality was not associated with expenditures.
Conclusions: Medicare payments around episodes of inpatient surgery are substantially higher at hospitals with high complications. These findings suggest that local, regional, and national efforts aimed at improving surgical quality may ultimately reduce costs and improve outcomes.
Figures
Comment in
-
The business of quality in surgery.Ann Surg. 2012 Jan;255(1):6-7. doi: 10.1097/SLA.0b013e31824135e4. Ann Surg. 2012. PMID: 22156930 No abstract available.
References
-
- Birkmeyer NJO, Birkmeyer JD. Strategies for Improving Surgical Quality - Should Payers Reward Excellence or Effort? [Miscellaneous] New England Journal of Medicine. 2006;354(8):864–870. - PubMed
-
- Birkmeyer JD, Dimick JB, Birkmeyer JD, Dimick JB. Potential benefits of the new Leapfrog standards: effect of process and outcomes measures.[see comment] Surgery. 2004 Jun;135(6):569–575. - PubMed
-
- Rosenthal MB, Frank RG, Li Z, Epstein AM. Early experience with pay for performance: From concept to practice. JAMA. 2005;294:1788–1793. - PubMed
-
- Share D, Campbell DA, Jr, Birkmeyer NJ, et al. How a regional collaborative of hospitals and physicians in Michigan cut costs and improved the quality of care. Health Aff (Millwood) 2011;30:636–645. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
