

Assessing mortality in women with hepatitis C virus and HIV using indirect markers of fibrosis
- PMID: 22156972
- PMCID: PMC3698040
- DOI: 10.1097/QAD.0b013e32834fa121
Assessing mortality in women with hepatitis C virus and HIV using indirect markers of fibrosis
Abstract
Objective: Co-infection with hepatitis C virus (HCV) is a major cause of morbidity and mortality in HIV-infected individuals. However, predictors of mortality are poorly defined and most studies have focused predominantly on co-infection in men. We evaluated whether two indirect markers of hepatic fibrosis, aspartate aminotransferase-to-platelet ratio index (APRI) and FIB-4 scores, were predictive of mortality in a well defined longitudinal cohort of HCV/HIV-co-infected women on HAART.
Methods: HCV/HIV-co-infected women on antiretroviral therapy enrolled in Women's Interagency HIV Study (WIHS), a National Institutes of Health-funded prospective, multicenter, cohort study of women with and at risk for HIV infection were included. Using Cox regression analysis, associations between APRI and FIB-4 with all-cause mortality were assessed.
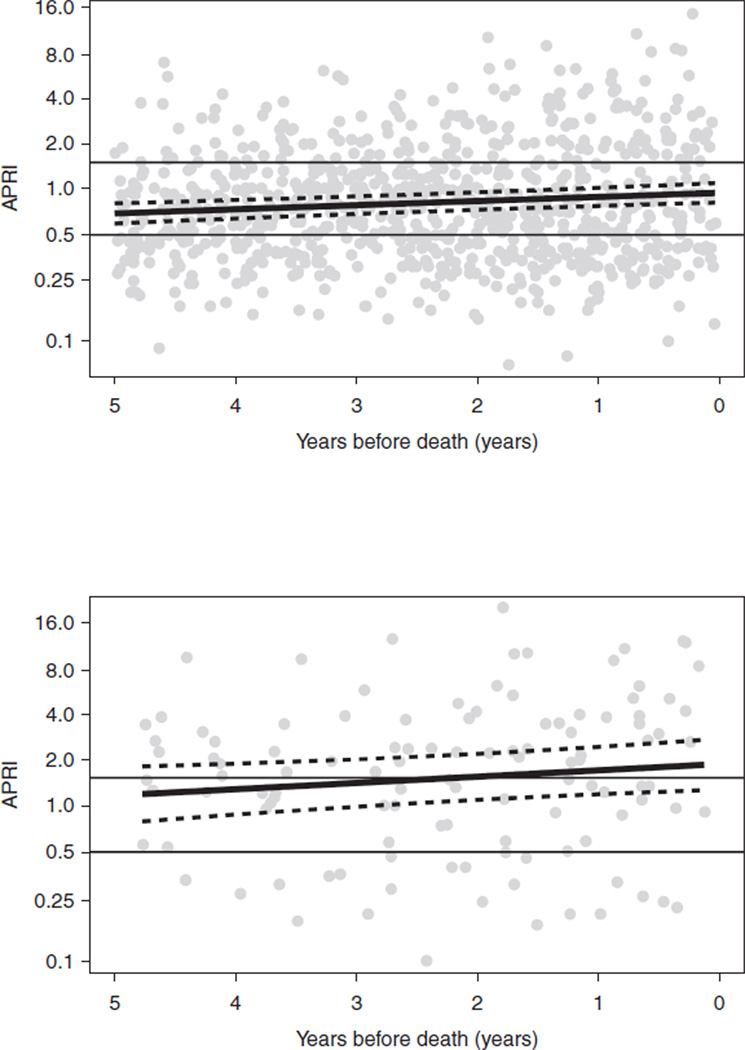
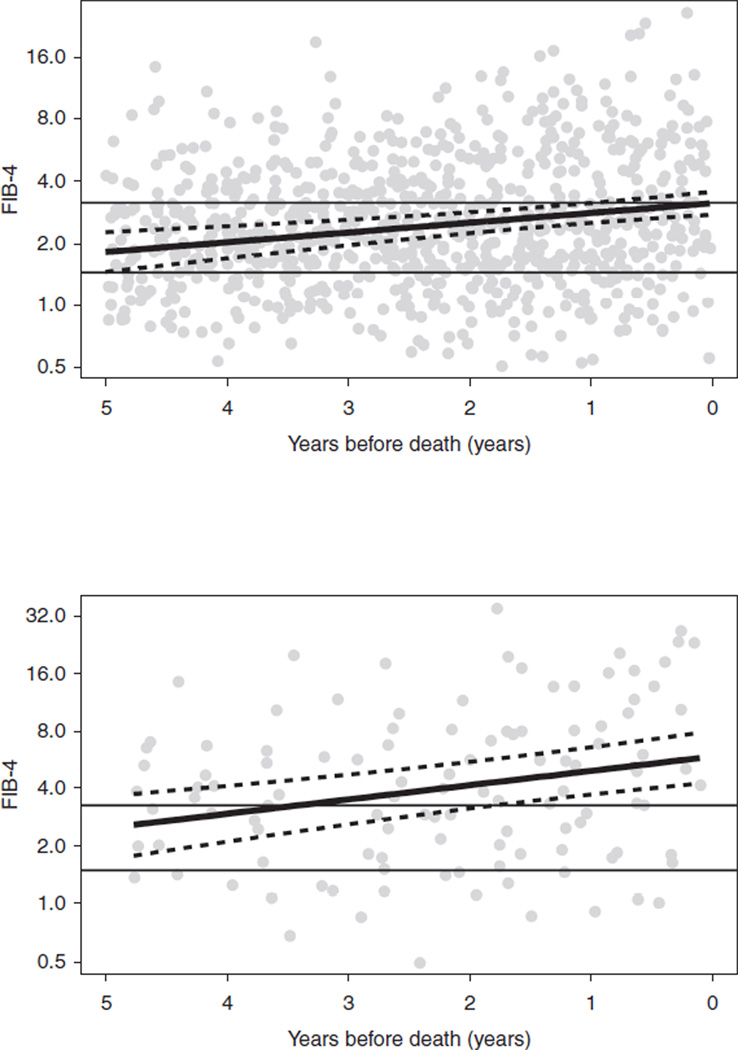
Results: Four hundred and fifty HCV/HIV-co-infected women, of whom 191 women died, had a median follow-up of 6.6 years and 5739 WIHS visits. Compared with women with low APRI or FIB-4 levels, severe fibrosis was significantly associated with an increased risk of all-cause mortality {APRI: hazard ratio 2.78 [95% confidence interval (CI) 1.87, 4.12]; FIB-4: hazard ratio 2.58 (95% CI 1.68, 3.95)}. Crude death rates per 1000 patient-years increased with increasing liver fibrosis: 34.8 for mild, 51.3 for moderate and 167.9 for severe fibrosis as measured by FIB-4. Importantly, both APRI and FIB-4 increased during the 5 years prior to death for all women: the slope of increase was greater for women dying a liver-related death compared with nonliver-related death.
Conclusion: Both APRI and FIB-4 are independently associated with all-cause mortality in HCV/HIV-co-infected women and may have clinical prognostic utility among women with HIV and HCV.
Conflict of interest statement
There are no conflicts of interest involved in this manuscript.
Figures
References
-
- Graham CS, Baden LR, Yu E, Mrus JM, Carnie J, Heeren T, et al. Influence of human immunodeficiency virus infection on the course of hepatitis C virus infection: a meta-analysis. Clin Infect Dis. 2001;33:562–569. - PubMed
-
- Benhamou Y, Bochet M, Di MV, Charlotte F, Azria F, Coutellier A, et al. Liver fibrosis progression in human immunodeficiency virus and hepatitis C virus coinfected patients. The Multivirc Group. Hepatology. 1999;30:1054–1058. - PubMed
-
- Kenny-Walsh E. Clinical outcomes after hepatitis C infection from contaminated anti-D immune globulin. Irish Hepatology Research Group. N Engl J Med. 1999;340:1228–1233. - PubMed
-
- Weber R, Sabin CA, Friis-Moller N, Reiss P, El Sadr WM, Kirk O, et al. Liver-related deaths in persons infected with the human immunodeficiency virus: the D:A:D study. Arch Intern Med. 2006;166:1632–1641. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- U01-AI-42590/AI/NIAID NIH HHS/United States
- U01 AI031834/AI/NIAID NIH HHS/United States
- K23 66943/PHS HHS/United States
- K24 AI078884/AI/NIAID NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- U01-AI-34994/AI/NIAID NIH HHS/United States
- U01-AI-35004/AI/NIAID NIH HHS/United States
- U01-AI-31834/AI/NIAID NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- R21 A1088361/PHS HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- U01-DH-32632/DH/BHP HRSA HHS/United States
- U01-AI-34993/AI/NIAID NIH HHS/United States
- R01 DK065515/DK/NIDDK NIH HHS/United States
- U01-AI-34989/AI/NIAID NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
- U01 AI042590/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Medical
