

Alteration of the nasal responses to influenza virus by tobacco smoke
- PMID: 22157158
- PMCID: PMC3305994
- DOI: 10.1097/ACI.0b013e32834ecc80
Alteration of the nasal responses to influenza virus by tobacco smoke
Abstract
Purpose of review: The purpose of this review is to highlight recent data regarding the impact of exposure to tobacco smoke on influenza virus infection. This is timely because of the continuing pattern for influenza to cause epidemics and pandemics.
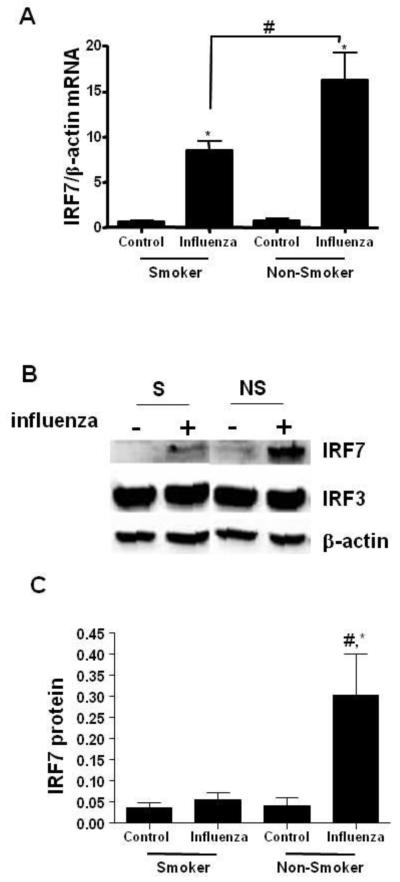
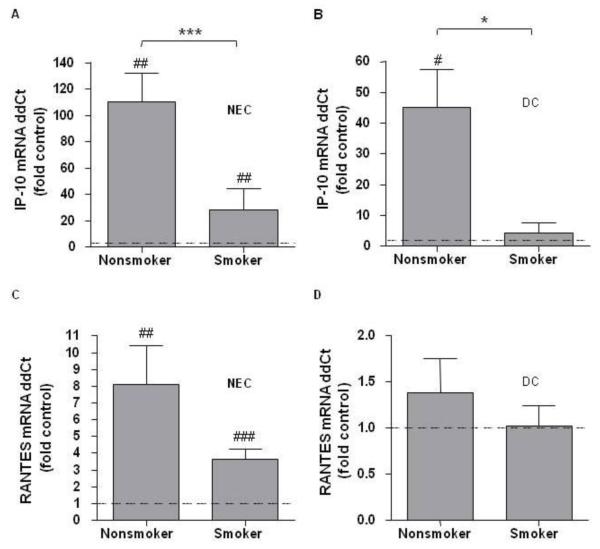
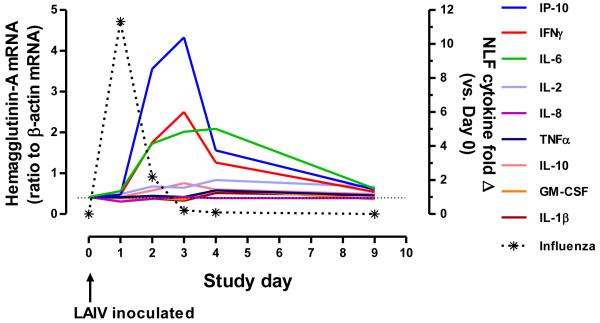
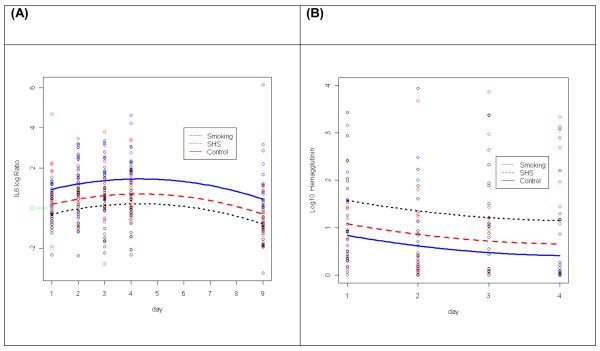
Recent findings: Experimental animal studies suggest tobacco smoke increases severity of respiratory disease with influenza. The interaction is complex and dependent on dose and chronicity of both virus and smoke exposure. Smoke-induced oxidant stress and suppression of innate immunity are mechanistic factors leading to worse disease. Experiments using human respiratory cells show that tobacco smoke increases viral replication through mechanisms including suppression of antiviral pathways and altered cytokine patterns in cell types with central roles in mucosal innate immunity, such as epithelium, dendritic cells, and natural killer cells. Studies also suggest a role for antioxidant strategies in reducing risk. Human volunteer studies using live attenuated influenza virus as a model appear to corroborate many of these findings.
Summary: Exposure to tobacco smoke remains extremely prevalent worldwide. Although avoidance of exposure is a primary goal, it is important to understand the mechanisms underlying increased infection risk with tobacco smoke and other pollutant exposures, so that novel preventive or treatment strategies can be developed.
Figures
Similar articles
-
Tobacco smoke exposure and altered nasal responses to live attenuated influenza virus.Environ Health Perspect. 2011 Jan;119(1):78-83. doi: 10.1289/ehp.1002258. Epub 2010 Oct 4. Environ Health Perspect. 2011. PMID: 20920950 Free PMC article.
-
Cigarette smoke inhibits BAFF expression and mucosal immunoglobulin A responses in the lung during influenza virus infection.Respir Res. 2015 Mar 14;16(1):37. doi: 10.1186/s12931-015-0201-y. Respir Res. 2015. PMID: 25849069 Free PMC article.
-
Cigarette smoke attenuates the RIG-I-initiated innate antiviral response to influenza infection in two murine models.Am J Physiol Lung Cell Mol Physiol. 2014 Dec 1;307(11):L848-58. doi: 10.1152/ajplung.00158.2014. Epub 2014 Sep 26. Am J Physiol Lung Cell Mol Physiol. 2014. PMID: 25260755 Free PMC article.
-
Role of γδ T cells in controlling viral infections with a focus on influenza virus: implications for designing novel therapeutic approaches.Virol J. 2020 Nov 12;17(1):174. doi: 10.1186/s12985-020-01449-0. Virol J. 2020. PMID: 33183352 Free PMC article. Review.
-
Influenza Virus RNA Synthesis and the Innate Immune Response.Viruses. 2021 Apr 28;13(5):780. doi: 10.3390/v13050780. Viruses. 2021. PMID: 33924859 Free PMC article. Review.
Cited by
-
Inhalation Toxicology of Vaping Products and Implications for Pulmonary Health.Int J Mol Sci. 2020 May 15;21(10):3495. doi: 10.3390/ijms21103495. Int J Mol Sci. 2020. PMID: 32429092 Free PMC article. Review.
-
Long-term smoking increases the need for acute care among asthma patients: a case control study.BMC Pulm Med. 2014 Jul 16;14:119. doi: 10.1186/1471-2466-14-119. BMC Pulm Med. 2014. PMID: 25030656 Free PMC article.
-
E-cigarette use results in suppression of immune and inflammatory-response genes in nasal epithelial cells similar to cigarette smoke.Am J Physiol Lung Cell Mol Physiol. 2016 Jul 1;311(1):L135-44. doi: 10.1152/ajplung.00170.2016. Epub 2016 Jun 10. Am J Physiol Lung Cell Mol Physiol. 2016. PMID: 27288488 Free PMC article.
-
Will chronic e-cigarette use cause lung disease?Am J Physiol Lung Cell Mol Physiol. 2015 Dec 15;309(12):L1398-409. doi: 10.1152/ajplung.00272.2015. Epub 2015 Sep 25. Am J Physiol Lung Cell Mol Physiol. 2015. PMID: 26408554 Free PMC article. Review.
-
Protective role of γδ T cells in cigarette smoke and influenza infection.Mucosal Immunol. 2018 May;11(3):894-908. doi: 10.1038/mi.2017.93. Epub 2017 Nov 1. Mucosal Immunol. 2018. PMID: 29091081 Free PMC article.
References
-
- Swerdlow DL, Finelli L, Bridges CB. H1N1 influenza pandemic: field and epidemiologic investigations in the United States at the start of the first pandemic of the 21st century. Clin Infect Dis. 2011 Jan 1;52(Suppl 1):S1–3. 2009. - PubMed
-
- Arcavi L, Benowitz NL. Cigarette smoking and infection. Arch Intern Med. 2004;164:2206–2216. - PubMed
-
- Kark JD, Lebiush M, Rannon L. Cigarette smoking as a risk factor for epidemic a(h1n1) influenza in young men. N Engl J Med. 1982;307:1042–1046. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
