

Membranoproliferative glomerulonephritis and C3 glomerulopathy: resolving the confusion
- PMID: 22157657
- PMCID: PMC4428602
- DOI: 10.1038/ki.2011.399
Membranoproliferative glomerulonephritis and C3 glomerulopathy: resolving the confusion
Abstract
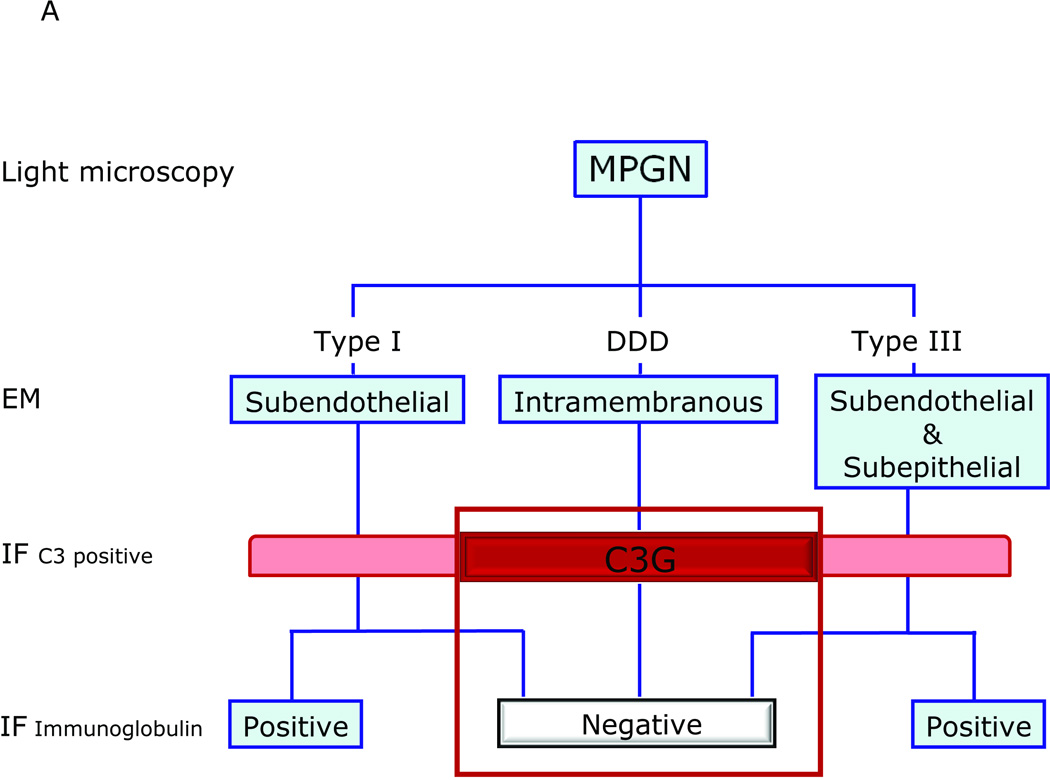
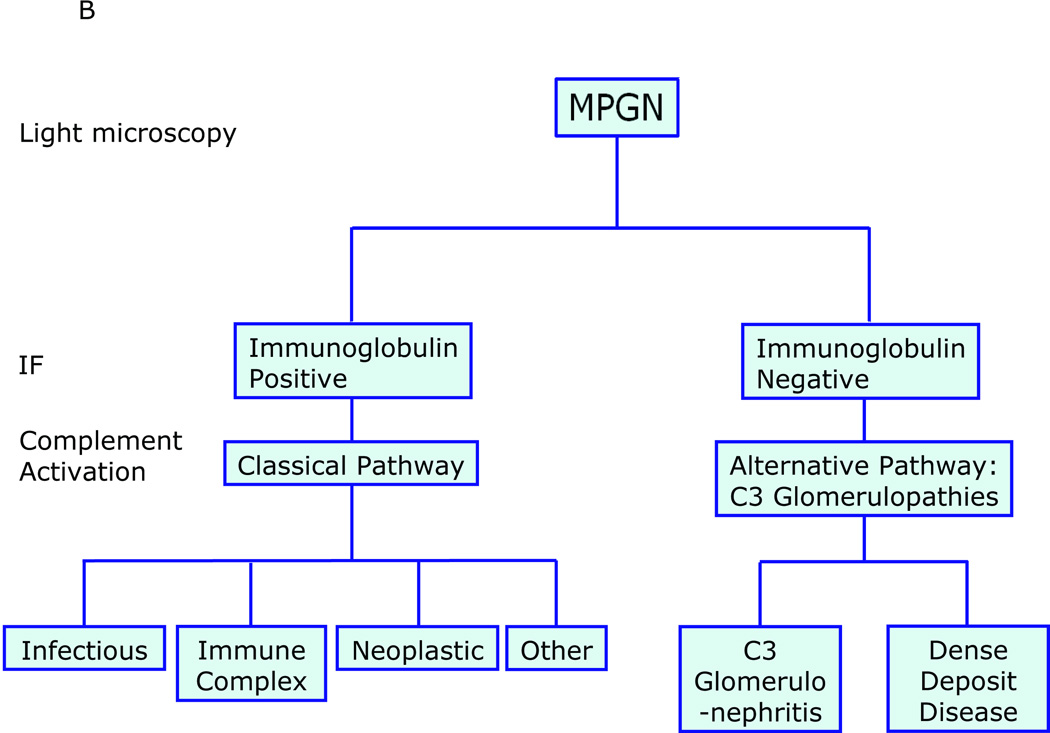
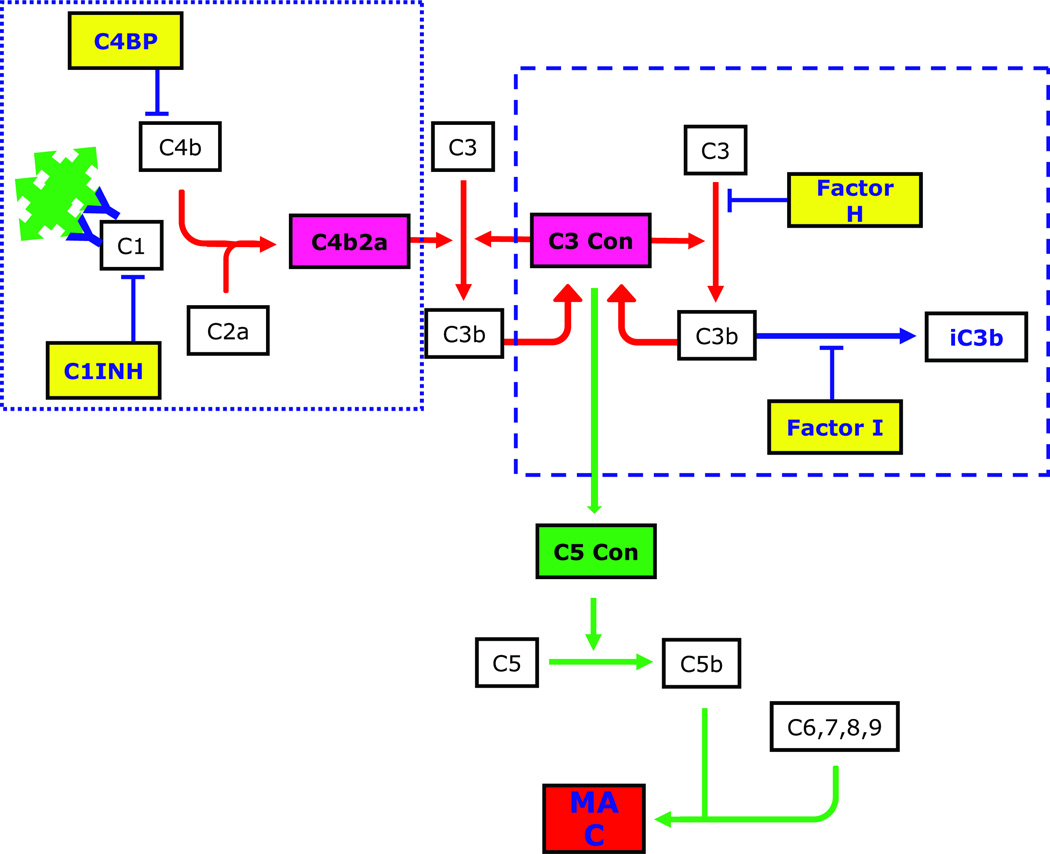
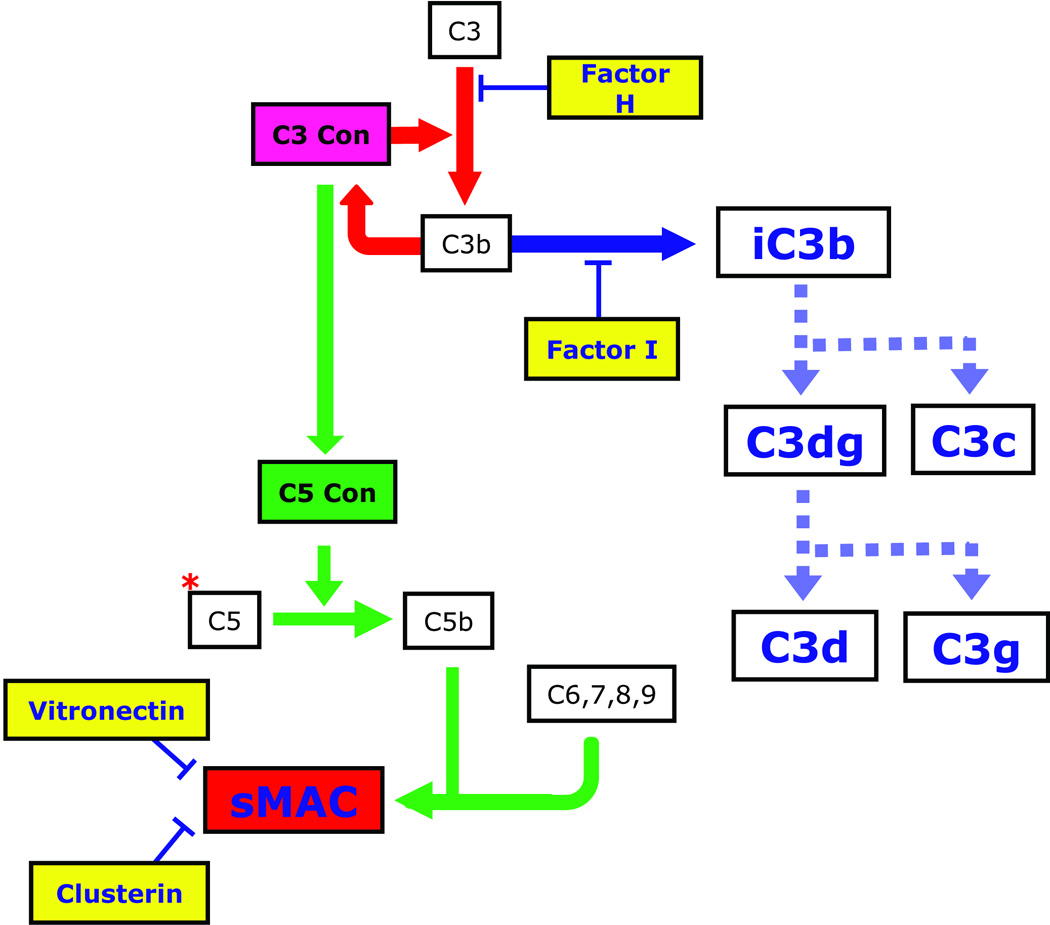
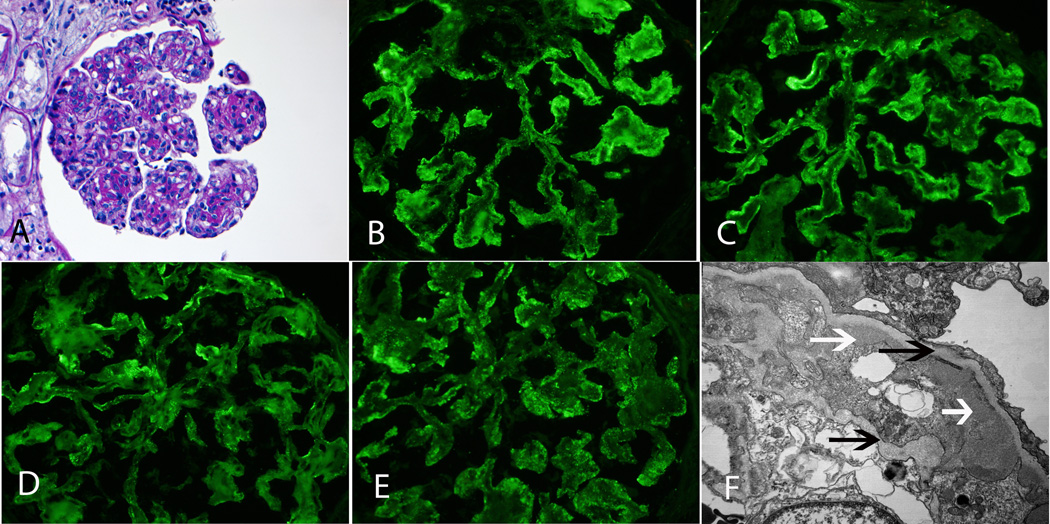
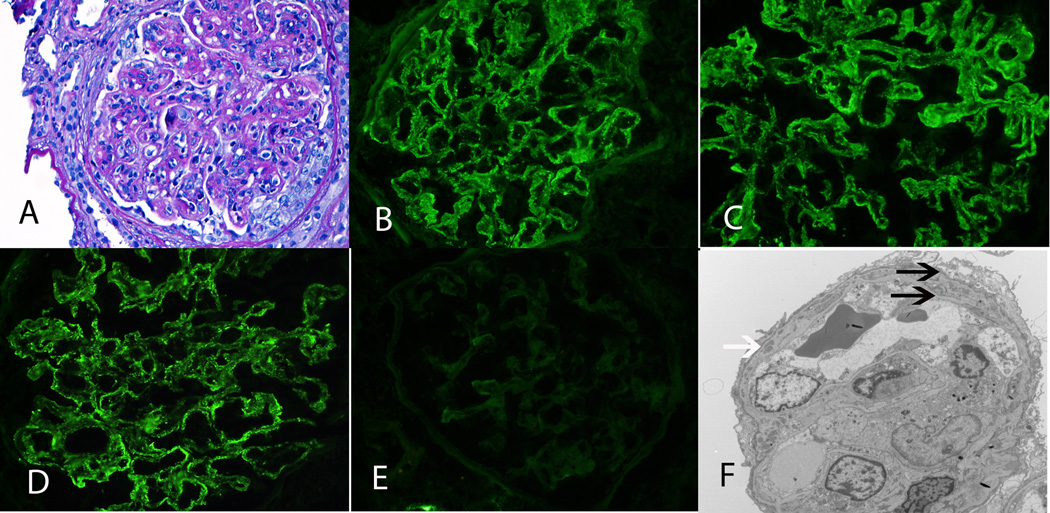
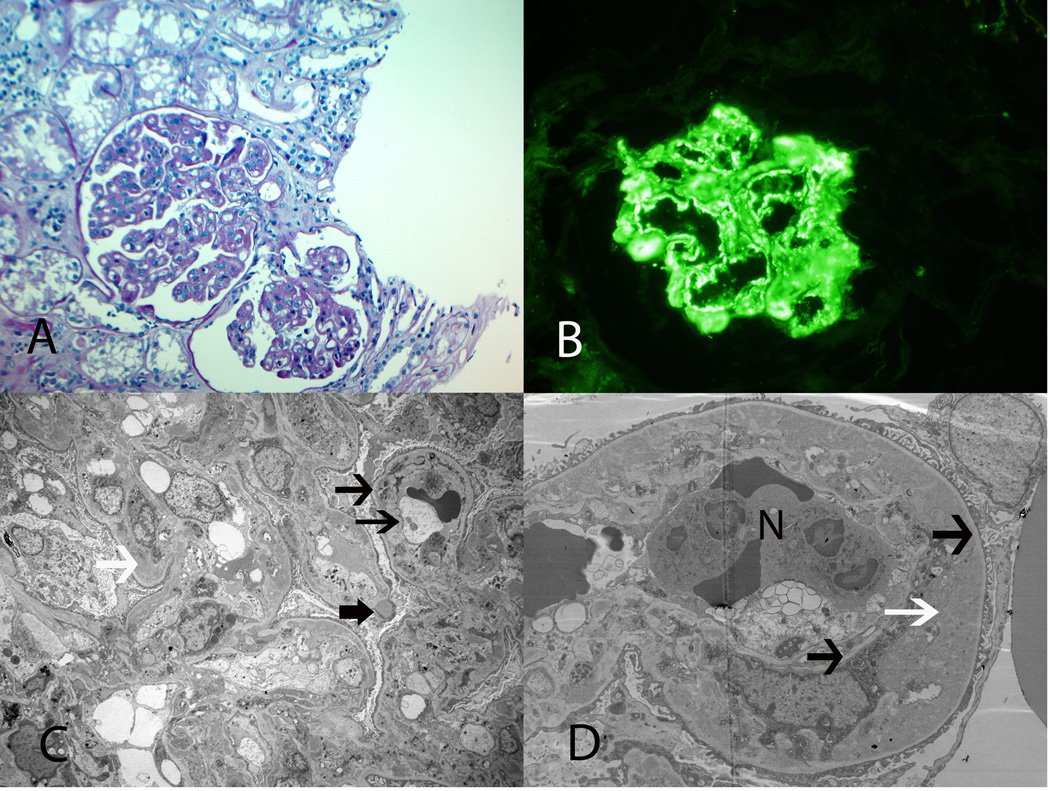
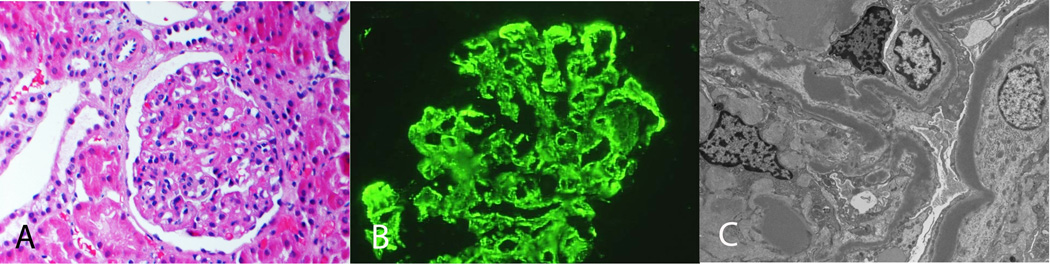
Membranoproliferative glomerulonephritis (MPGN) denotes a general pattern of glomerular injury that is easily recognized by light microscopy. With additional studies, MPGN subgrouping is possible. For example, electron microscopy resolves differences in electron-dense deposition that are classically referred to as MPGN type I (MPGN I), MPGN II, and MPGN III, while immunofluorescence typically detects immunoglobulins in MPGN I and MPGN III but not in MPGN II. All three MPGN types stain positive for complement component 3 (C3). Subgrouping has led to unnecessary confusion, primarily because immunoglobulin-negative MPGN I and MPGN III are more common than once recognized. Together with MPGN II, which is now called dense deposit disease, immunoglobulin-negative, C3-positive glomerular diseases fall under the umbrella of C3 glomerulopathies (C3G). The evaluation of immunoglobulin-positive MPGN should focus on identifying the underlying trigger driving the chronic antigenemia or circulating immune complexes in order to begin disease-specific treatment. The evaluation of C3G, in contrast, should focus on the complement cascade, as dysregulation of the alternative pathway and terminal complement cascade underlies pathogenesis. Although there are no disease-specific treatments currently available for C3G, a better understanding of their pathogenesis would set the stage for the possible use of anti-complement drugs.
Figures
Comment in
-
The many faces of C3 glomerulopathy.Kidney Int. 2012 Sep;82(5):611; author reply 611. doi: 10.1038/ki.2012.220. Kidney Int. 2012. PMID: 22892860 No abstract available.
References
-
- Anders D, Thoenes W. Basement membrane changes in membranoproliferative glomerulonephritis: a light and electron microscopic study. Virchows Arch Pathol Anat. 1975;369:87–109. - PubMed
-
- Habib R, Kleinknecht C, Gubler MC, Levy M. Idiopathic membranoproliferative glomerulonephritis in children. Report of 105 cases. Clin Nephrol. 1973;1:194–214. - PubMed
-
- Jackson EC, McAdams AJ, Strife CF, et al. Differences between membranoproliferative glomerulonephritis types I and III in clinical presentation, glomerular morphology and complement pertubation. Am J Kidney Dis. 1987;9:115–120. - PubMed
-
- Strife CF, McEnery PT, McAdams AJ, et al. Membranoproliferative glomerulonephritis with disruption of the glomerular basement membrane. Clin Nephrol. 1977;7:65–72. - PubMed
-
- Levy M, Gubler M-C, Sich M, et al. Immunopathology of membranoproliferative glomerulonephritis with subendothelial deposits (Type I MPGN) Clin Immunol Immunopathol. 1978;10:477–492. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
