

Validation study of oxford classification of IgA nephropathy: the significance of extracapillary proliferation
- PMID: 22157710
- PMCID: PMC3255377
- DOI: 10.2215/CJN.02890311
Validation study of oxford classification of IgA nephropathy: the significance of extracapillary proliferation
Abstract
BACKGROUND AND OBJECTIVES The Oxford classification of IgA nephropathy (IgAN) includes mesangial hypercellularity, endocapillary hypercellularity, segmental glomerulosclerosis (S), and tubular atrophy/interstitial fibrosis (T) as prognosticators. The value of extracapillary proliferation (Ex) was not addressed. Because the Oxford classification excludes patients with urinary protein <0.5 g/d and eGFR <30 ml/min per 1.73 m(2) at biopsy, the significance of Ex should be confirmed by validation cohorts that include more rapidly progressive cases. We present such a study.
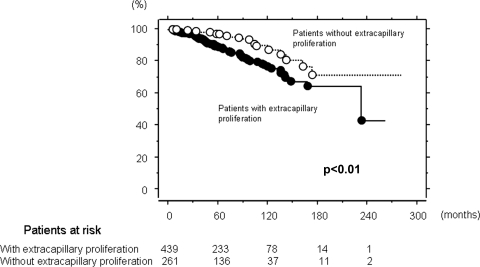
Design, setting, participants, & measurements: The significance of pathologic features for development end-stage renal failure (ESRF) was examined by multivariate analysis in 702 patients with IgAN. The association of Ex with kidney survival was examined by univariate analysis in 416 patients who met the Oxford criteria and 286 who did not, separately.
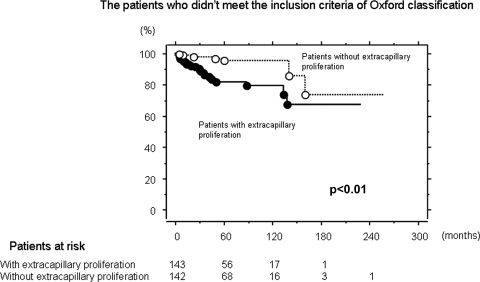
Results: In a multivariate model, S and T were significantly associated with ESRF. With addition of Ex, not S but Ex was significant for ESRF. In univariate analysis, kidney survival was significantly lower in patients with Ex than in those without, in patients who did not meet the Oxford criteria, but such a difference was not found in patients who met it.
Conclusions: The prognostic significance of Ex was evident in our cohort. It seems that Ex did not emerge from the Oxford classification as a prognosticator because of exclusion of severe cases (eGFR <30 ml/min per 1.73 m(2)). We suggest that extracapillary proliferation be included in the next version of the Oxford classification of IgAN to widen the scope of the classification.
Figures

Similar articles
-
The use of the Oxford classification of IgA nephropathy to predict renal survival.Clin J Am Soc Nephrol. 2011 Oct;6(10):2384-8. doi: 10.2215/CJN.01170211. Epub 2011 Sep 1. Clin J Am Soc Nephrol. 2011. PMID: 21885791 Free PMC article.
-
Validation study of Oxford Classification of IgA Nephropathy: the significance of extracapillary hypercellularity and mesangial IgG immunostaining.Pathol Int. 2016 Aug;66(8):453-9. doi: 10.1111/pin.12442. Epub 2016 Jul 21. Pathol Int. 2016. PMID: 27439692
-
Validation of the Oxford classification of IgA nephropathy in cohorts with different presentations and treatments.Kidney Int. 2014 Oct;86(4):828-36. doi: 10.1038/ki.2014.63. Epub 2014 Apr 2. Kidney Int. 2014. PMID: 24694989 Free PMC article.
-
Extracapillary proliferation in IgA nephropathy; recent findings and new ideas.J Nephropathol. 2015 Jan;4(1):1-5. doi: 10.12860/jnp.2015.01. Epub 2015 Jan 1. J Nephropathol. 2015. PMID: 25657978 Free PMC article. Review.
-
Oxford classification of immunoglobulin A nephropathy: an update.Curr Opin Nephrol Hypertens. 2013 May;22(3):281-6. doi: 10.1097/MNH.0b013e32835fe65c. Curr Opin Nephrol Hypertens. 2013. PMID: 23518465 Review.
Cited by
-
Contemporary review of IgA nephropathy.Front Immunol. 2024 Aug 12;15:1436923. doi: 10.3389/fimmu.2024.1436923. eCollection 2024. Front Immunol. 2024. PMID: 39188719 Free PMC article. Review.
-
Impact of tonsillectomy combined with steroid pulse therapy on immunoglobulin A nephropathy depending on histological classification: a multicenter study.Clin Exp Nephrol. 2016 Feb;20(1):50-7. doi: 10.1007/s10157-015-1131-1. Epub 2015 Jun 9. Clin Exp Nephrol. 2016. PMID: 26055039
-
Role of immunosuppressive therapy and predictors of therapeutic effectiveness and renal outcome in IgA nephropathy with proteinuria.Arch Med Sci. 2015 Apr 25;11(2):332-9. doi: 10.5114/aoms.2015.50965. Epub 2015 Apr 23. Arch Med Sci. 2015. PMID: 25995749 Free PMC article.
-
Comment on: Association of Proteinuria with Various Clinical Findings and Morphologic Variables of Oxford Classification in Immunoglobulin A Nephropathy Patients.Int J Prev Med. 2014 Oct;5(10):1349-50. Int J Prev Med. 2014. PMID: 25400897 Free PMC article. No abstract available.
-
The Japanese Histologic Classification and T-score in the Oxford Classification system could predict renal outcome in Japanese IgA nephropathy patients.Clin Exp Nephrol. 2017 Dec;21(6):986-994. doi: 10.1007/s10157-017-1393-x. Epub 2017 Mar 27. Clin Exp Nephrol. 2017. PMID: 28349230
References
-
- Alamartine E, Sabatier JC, Berthoux FC: Comparison of pathological lesions on repeated renal biopsies in 73 patients with primary IgA glomerulonephritis: Value of quantitative scoring and approach to final prognosis. Clin Nephrol 34: 45–51, 1990 - PubMed
-
- Radford MG, Jr, Donadio JV, Jr, Bergstralh EJ, Grande JP: Predicting renal outcome in IgA nephropathy. J Am Soc Nephrol 8: 199–207, 1997 - PubMed
-
- Katafuchi R, Kiyoshi Y, Oh Y, Uesugi N, Ikeda K, Yanase T, Fujimi S: Glomerular score as a prognosticator in IgA nephropathy: Its usefulness and limitation. Clin Nephrol 49: 1–8, 1998 - PubMed
-
- Lee SM, Rao VM, Franklin WA, Schiffer MS, Aronson AJ, Spargo BH, Katz AI: IgA nephropathy: Morphologic predictors of progressive renal disease. Hum Pathol 13: 314–322, 1982 - PubMed
-
- Haas M: Histologic subclassification of IgA nephropathy: A clinicopathologic study of 244 cases. Am J Kidney Dis 29: 829–842, 1997 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
