

Embryonal rhabdomyosarcoma of the uterine cervix: a report of 14 cases and a discussion of its unusual clinicopathological associations
- PMID: 22157934
- PMCID: PMC5031244
- DOI: 10.1038/modpathol.2011.185
Embryonal rhabdomyosarcoma of the uterine cervix: a report of 14 cases and a discussion of its unusual clinicopathological associations
Abstract
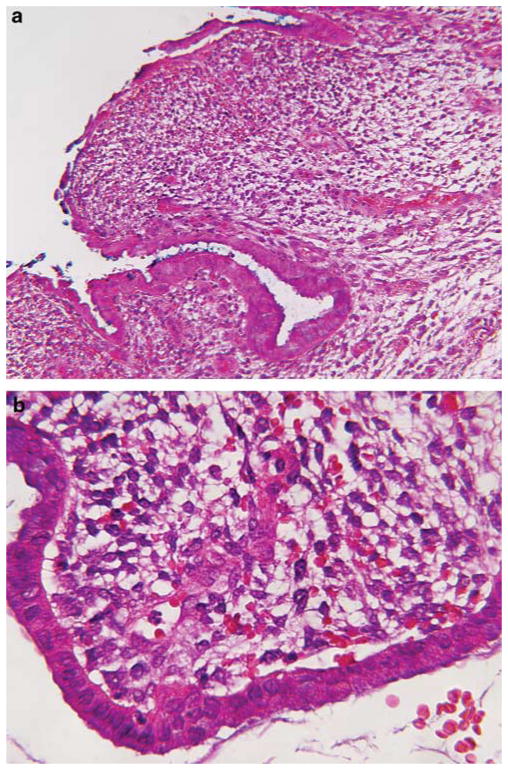
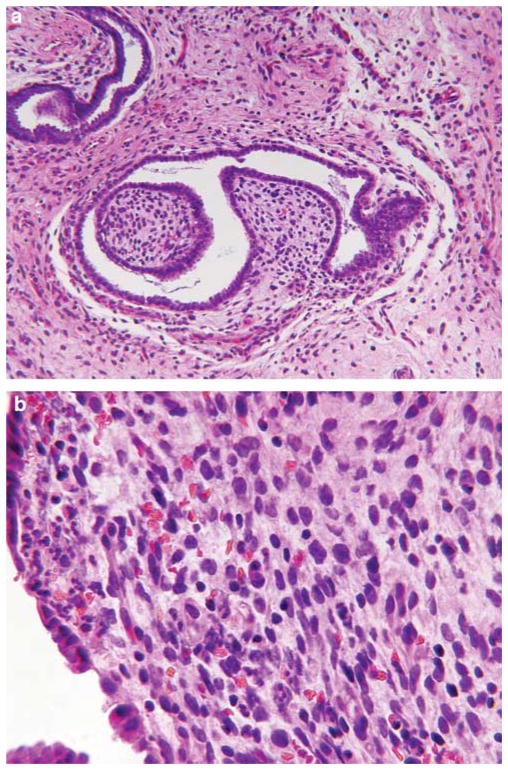
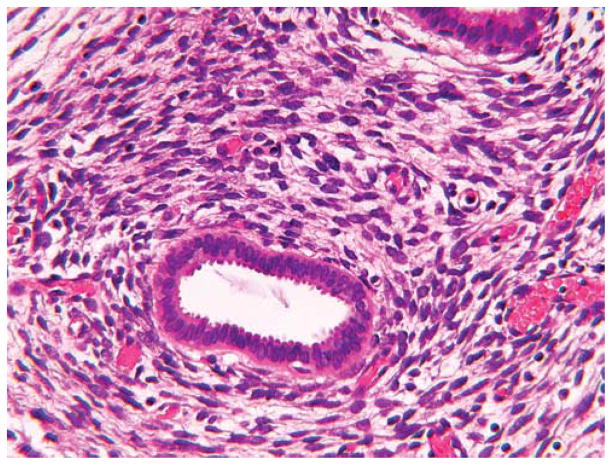
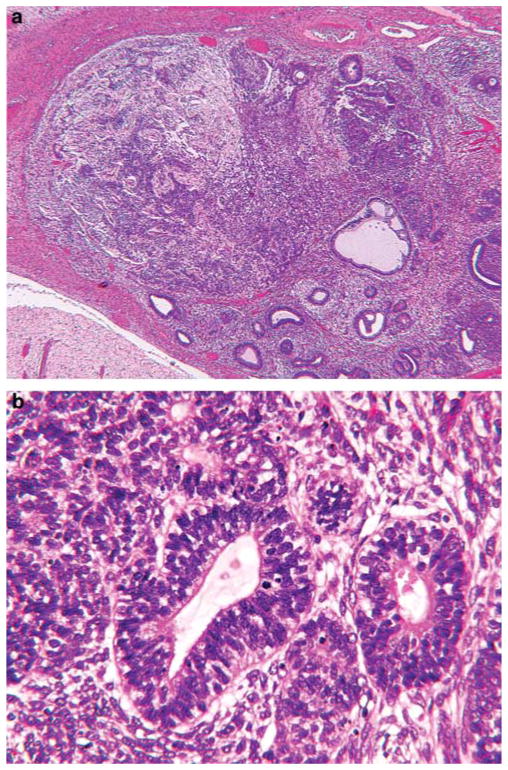
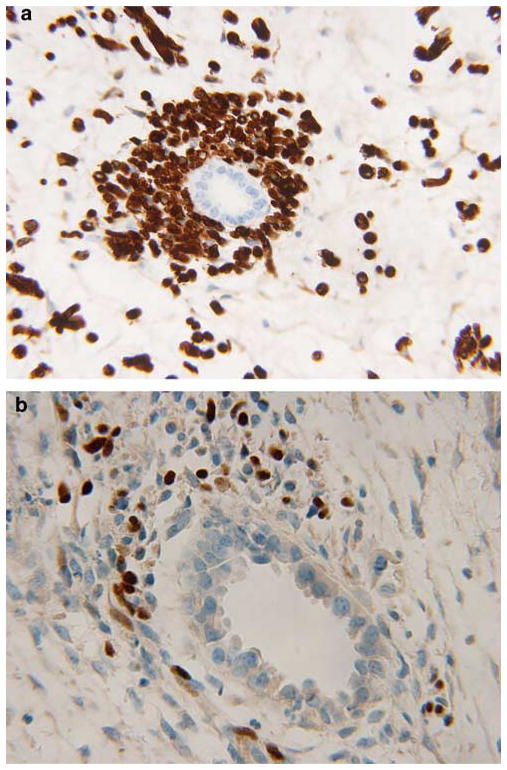
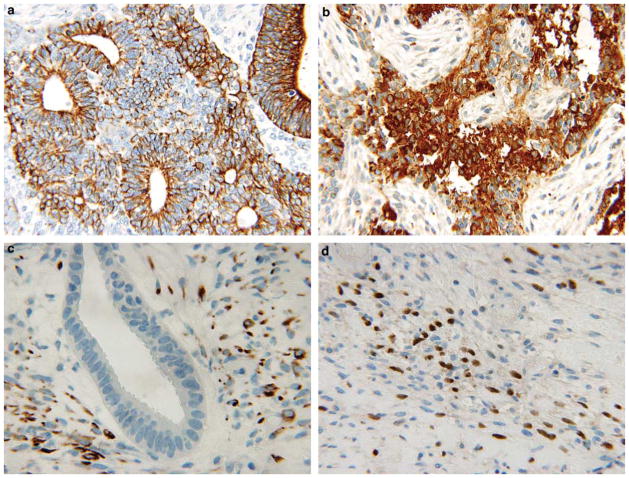
Embryonal rhabdomyosarcoma of the uterine cervix is an uncommon presentation of the most common soft-tissue sarcoma in the first decades of life. Unlike embryonal rhabdomyosarcoma in other anatomic sites, in which 70-80% of cases present before 9 years of age, the average age in our series of 14 cervical cases was 12.4 years (median, 13 years), with an age range of 9 months to 32 years at diagnosis. Of the 14 cases, 12 presented as a polyp at the cervical os; two patients had an infiltrative mass in the cervix without a botryoid polyp. The polyps measured 1.5-5 cm and all had the histopathological pattern of the sarcoma botryoides variant of embryonal rhabdomyosarcoma, with condensations of primitive and differentiated rhabdomyoblasts beneath the surface epithelium and around endocervical glands. Nodules of benign-appearing cartilage were present in the stroma of six cases (43%). One of the embyronal rhabdomyosarcomas from the youngest patient, 9 months old, also had a distinctive microscopic focus of immature tubular profiles in a primitive stroma; these tubules expressed epithelial and neuroendocrine markers. Two patients had a pleuropulmonary blastoma, one diagnosed 9 years before the embryonal rhabdomyosarcoma of the cervix and the other recognized synchronously. This latter 9-year old had a DICER1 germline mutation. One patient presented with hirsutism and had a Sertoli-Leydig cell tumor, an incidentally detected cervical embryonal rhabdomyosarcoma, and nodular hyperplasia of the thyroid. Although a pleuropulmonary blastoma was not documented in the latter patient, ovarian sex-cord stromal tumors and nodular hyperplasia of the thyroid are manifestations of the pleuropulmonary blastoma family tumor and dysplasia syndrome (OMIM 601200). Embryonal rhabdomyosarcoma of the cervix must be distinguished from other rare entities, including adenosarcoma, malignant mixed Mullerian tumor and low-grade stromal sarcoma, as the former has a better prognosis; 12 of our 14 patients remain disease-free following conservative surgery and chemotherapy. Our study suggests that cervical embryonal rhabdomyosarcoma may be another pathological manifestation in the spectrum of extrapulmonary pathology in the setting of pleuropulmonary blastoma.
Conflict of interest statement
Disclosure/conflict of interest The authors declare no conflict of interest.
Figures






References
-
- Dehner LP. Soft tissues. In: Stocker TJ, Dehner LP, Husain A, editors. Stocker and Dehner’s Pediatric Pathology. 3. Wolter Kluwer–Lippincott Williams & Wilkins; Philadelphia: 2011. pp. 1079–1087.
-
- Leuschner I, Harms D, Mattke A, et al. Rhabdomyosarcoma of the urinary bladder and vagina. A clinicopathologic study with emphasis on recurrent disease: a report from the Kiel Pediatric Tumor Registry and the German CWS Study. Am J Surg Pathol. 2001;25:856–864. - PubMed
-
- Herzog CE. Overview of sarcomas in the adolescent and young adult population. J Pediatr Hematol Oncol. 2005;27:215–218. - PubMed
