

Evaluation of visual acuity measurements after autorefraction vs manual refraction in eyes with and without diabetic macular edema
- PMID: 22159173
- PMCID: PMC3489033
- DOI: 10.1001/archophthalmol.2011.377
Evaluation of visual acuity measurements after autorefraction vs manual refraction in eyes with and without diabetic macular edema
Abstract
Objective: To compare visual acuity (VA) scores after autorefraction vs manual refraction in eyes of patients with diabetes mellitus and a wide range of VAs.
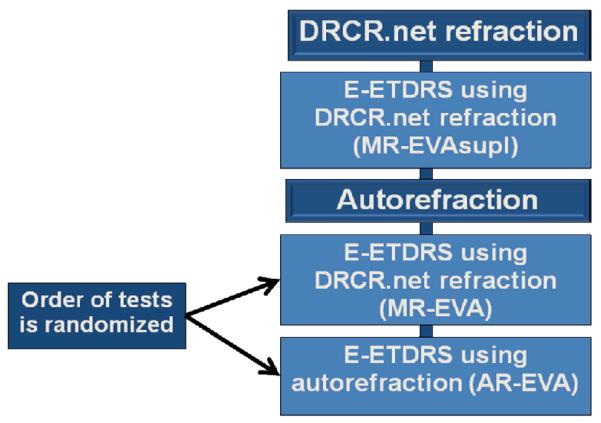
Methods: The letter score from the Electronic Visual Acuity (EVA) test from the electronic Early Treatment Diabetic Retinopathy Study was measured after autorefraction (AR-EVA score) and after manual refraction (MR-EVA score), which is the research protocol of the Diabetic Retinopathy Clinical Research Network. Testing order was randomized, study participants and VA examiners were masked to refraction source, and a second EVA test using an identical supplemental manual refraction (MR-EVAsuppl score) was performed to determine test-retest variability.
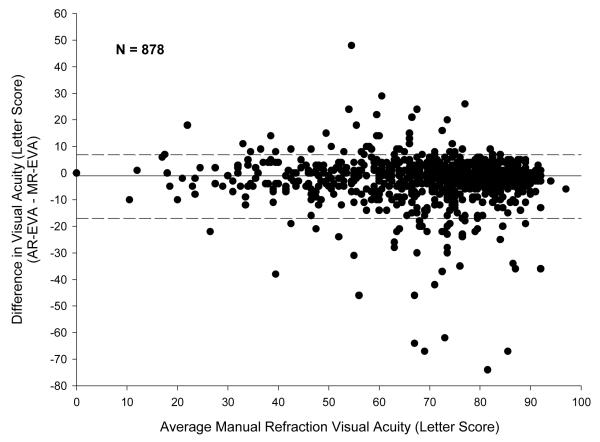
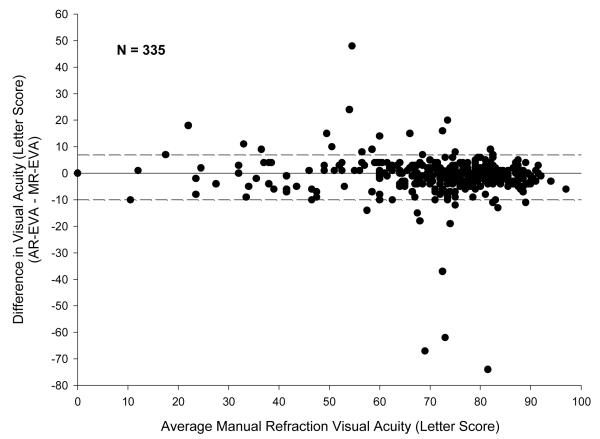
Results: In 878 eyes of 456 study participants, the median MR-EVA score was 74 (Snellen equivalent, approximately 20/32). The spherical equivalent was often similar for manual refraction and autorefraction (median difference, 0.00; 5th-95th percentile range, -1.75 to 1.13 diopters). However, on average, the MR-EVA scores were slightly better than the AR-EVA scores, across the entire VA range. Furthermore, the variability between the AR-EVA scores and the MR-EVA scores was substantially greater than the test-retest variability of the MR-EVA scores (P < .001). The variability of differences was highly dependent on the autorefractor model.
Conclusions: Across a wide range of VAs at multiple sites using a variety of autorefractors, VA measurements tend to be worse with autorefraction than manual refraction. Differences between individual autorefractor models were identified. However, even among autorefractor models that compare most favorably with manual refraction, VA variability between autorefraction and manual refraction is higher than the test-retest variability of manual refraction. The results suggest that, with current instruments, autorefraction is not an acceptable substitute for manual refraction for most clinical trials with primary outcomes dependent on best-corrected VA.
Figures


References
-
- Ferris FL, 3rd, Kassoff A, Bresnick GH, Bailey I. New visual acuity charts for clinical research. Am J Ophthalmol. 1982;94:91–6. - PubMed
-
- Early Treatment Diabetic Retinopathy Study Research Group Early treatment diabetic retinopathy study design and baseline patient characteristics. ETDRS report number 7. Ophthalmology. 1991;98:741–56. - PubMed
-
- Pesudovs K, Weisinger HS. A comparison of autorefractor performance. Optom Vis Sci. 2004;81(7):554–8. - PubMed
-
- Cornsweet TN, Crane HD. Servo-controlled infrared optometer. J Opt Soc Am. 1970;60(4):548–54. - PubMed
-
- Knoll HA, Mohrman R. The ophthalmetron, principles and operation. Am J Optom Arch Am Acad Optom. 1972;49(2):122–8. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
