

Variations in the use of internal fixation for distal radial fracture in the United States medicare population
- PMID: 22159850
- PMCID: PMC3226419
- DOI: 10.2106/JBJS.J.012802
Variations in the use of internal fixation for distal radial fracture in the United States medicare population
Abstract
Background: Distal radial fractures affect an estimated 80,000 elderly Americans each year. Although the use of internal fixation for the treatment of distal radial fractures is becoming increasingly common, there have been no population-based studies to explore the dissemination of this technique. The aims of our study were to determine the current use of internal fixation for the treatment of distal radial fractures in the Medicare population and to examine regional variations and other factors that influence use of this treatment. We hypothesized that internal fixation of distal radial fractures would be used less commonly in male and black populations compared with other populations because the prevalence of osteoporosis is lower in these populations, and that use of internal fixation would be correlated with the percentage of the patients who were treated by a hand surgeon in a particular region.
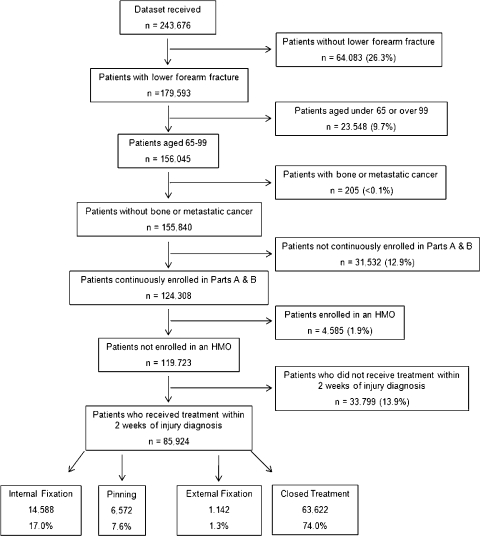
Methods: We performed an analysis of complete 2007 Medicare data to determine the percentage of distal radial fractures that were treated with internal fixation in each hospital referral region. We then analyzed the association of patient and physician factors with the type of fracture treatment received, both nationally and within each hospital referral region.
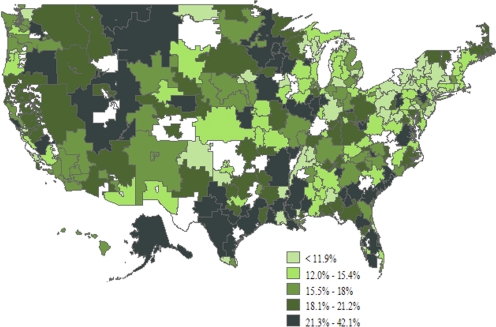
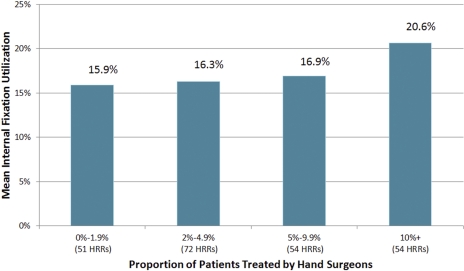
Results: We identified 85,924 Medicare beneficiaries with a closed distal radial fracture who met the inclusion criteria, and 17.0% of these patients were treated with internal fixation. Fractures were significantly less likely to be treated with internal fixation in men than in women (odds ratio, 0.84; 95% confidence interval, 0.80 to 0.89) and in black patients than in white patients (odds ratio, 0.74; 95% confidence interval, 0.65 to 0.85). Patients were more likely to be treated with internal fixation rather than with another treatment if they were treated by a hand surgeon than if they were treated by an orthopaedic surgeon who was not a hand surgeon (odds ratio, 2.49; 95% confidence interval, 2.29 to 2.70). Use of internal fixation ranged from 4.6% to 42.1% (nearly a ten-fold difference) among hospital referral regions. The percentage of patients treated with internal fixation within a hospital referral region was positively correlated with the percentage of patients in that region who were treated by a hand surgeon (correlation coefficient, 0.34; p < 0.0001).
Conclusions: The use of internal fixation for the treatment of a distal radial fracture differs widely among geographical regions and patient populations. Such variations highlight the need for improved comparative-effectiveness data to guide the treatment of this fracture.
Figures
References
-
- Ohsfeldt RL, Borisov NN, Sheer RL. Fragility fracture-related direct medical costs in the first year following a nonvertebral fracture in a managed care setting. Osteoporos Int. 2006;17:252-8 - PubMed
-
- Ray NF, Chan JK, Thamer M, Melton LJ., 3rd Medical expenditures for the treatment of osteoporotic fractures in the United States in 1995: report from the National Osteoporosis Foundation. J Bone Miner Res. 1997;12:24-35 - PubMed
-
- US Census Bureau Projected population of the United States, by age and sex: 2000-2050. http://www.census.gov/population/www/projections/usinterimproj/natprojta.... Accessed 2010 Apr 5
-
- Mackenney PJ, McQueen MM, Elton R. Prediction of instability in distal radial fractures. J Bone Joint Surg Am. 2006;88:1944-51 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
