

doi: 10.1007/s13181-011-0198-7.
Prediction of drug response and safety in clinical practice
Affiliations
- PMID: 22160757
- PMCID: PMC3550218
- DOI: 10.1007/s13181-011-0198-7
Item in Clipboard
Prediction of drug response and safety in clinical practice
J Med Toxicol.
2012 Mar.
Abstract
Many clinicians hoped that the completion of the Human Genome Project would result in "individualized drug therapy," i.e., determining the right medication at the right dose 100% of the time based upon the individual's genetics. The pharmacogenomic prediction of drug efficacy and safety has not become a reality due to continuing realization of the complexity dictating the human-drug interaction. New methods of metabolomics, proteomics, and transcriptomics that account for this complexity hold promise for translational researchers hoping to increase drug efficacy and decrease drug toxicity.
Figures
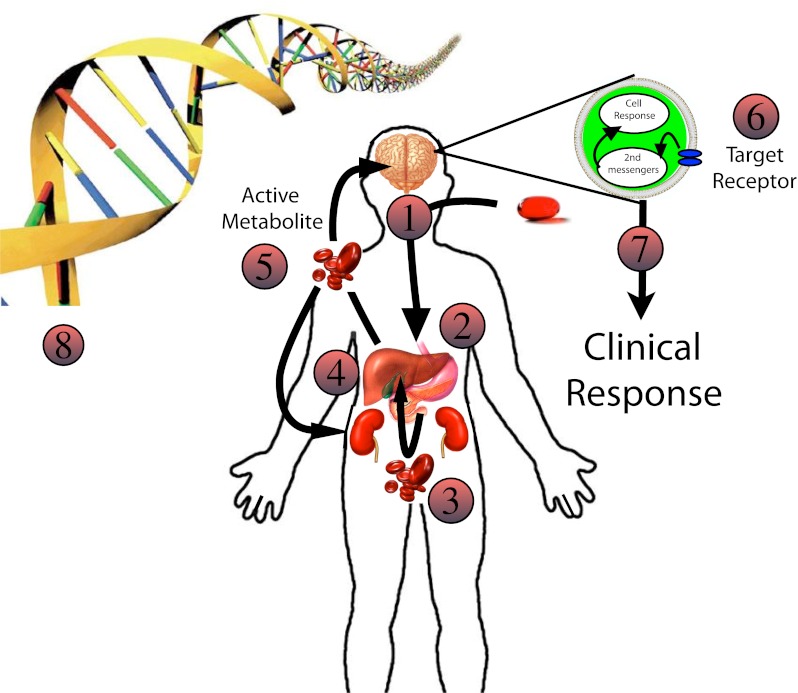
The complexity of drug response in the individual patient: 1 Drug ingested—Variations in drug dose may affect efficacy. 2 Drug absorption—Variations in the local gastrointestinal environment (acid concentration, absorption surface, bacteria, gut motility, etc) may affect the amount of drug available for absorption. 3 Translocation into blood—Drug crosses the intestinal epithelium, some is metabolized at the intestinal brush border; then the drug and its metabolites enter the portal vein and travel to the liver. Polymorphisms in drug transporters as well as changes in blood flow may affect drug delivery to the liver. 4 Hepatic DMEs—If there is low enzyme capacity, the drug may be shunted to other DMEs resulting in alternative metabolites with variable activity. Drug inhibitors or inducers may change the percentages of drug metabolites entering systemic circulation. 5 Systemic circulation—After leaving the liver, drug metabolites are sent to target organs and cleared by the kidneys. Blood flow and transporters may affect the amount of active metabolite reaching the drug target and the subsequent drug clearance. 6 Target receptor—The expression of drug target receptors may affect the clinical response. Variations in overall number, affinity for the drug, and the presence of inhibitors may result in variable clinical response. 7 Clinical response—May be affected by upstream variations as well as changes in downstream second messenger systems leading to variable phenotypic response. 8 Genetic polymorphism—Each step may be effected by gene polymorphism. In addition, local DNA/RNA environmental factors may affect transcription and translation. Given that each step is dependent on multiple genes, the range of phenotypes expressed is enormous for complex diseases. Ultimately, it is unlikely for identification of single mutations to determine individual patient phenotypes
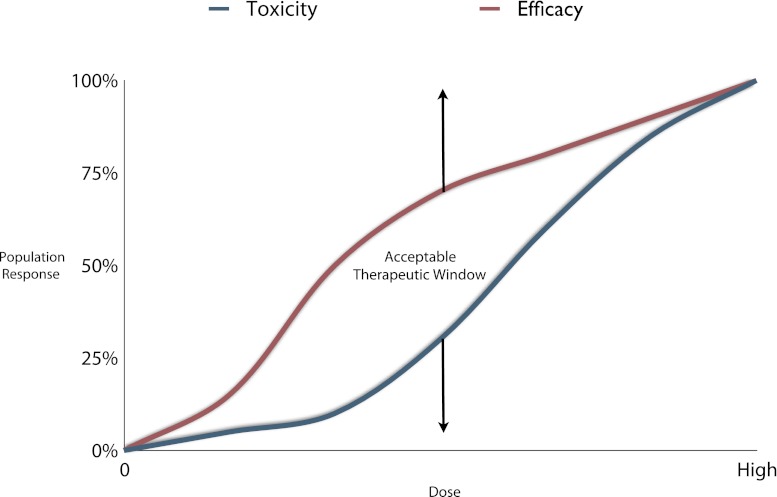
Population response versus toxicity: The area between the curves represents the therapeutic range in which efficacy is outweighed by the toxicity. At higher doses, the efficacy and toxicity lines begin to converge making the risk of toxicity not worth the increased efficacy. BSPs may allow exclusion of patients at risk of toxicity and allow for increased doses in drug-resistant patients. This can increase the area between these lines thereby increasing efficacy and decreasing toxicity for a specific drug
References
-
- Ieiri I, Higuchi S, Sugiyama Y. Genetic polymorphisms of uptake (OATP1B1, 1B3) and efflux (MRP2, BCRP) transporters: implications for inter-individual differences in the pharmacokinetics and pharmacodynamics of statins and other clinically relevant drugs. Expert Opin Drug Metab Toxicol. 2009;5(7):703–729. doi: 10.1517/17425250902976854. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
