

Parent training interventions for Attention Deficit Hyperactivity Disorder (ADHD) in children aged 5 to 18 years
- PMID: 22161373
- PMCID: PMC6544776
- DOI: 10.1002/14651858.CD003018.pub3
Parent training interventions for Attention Deficit Hyperactivity Disorder (ADHD) in children aged 5 to 18 years
Abstract
Background: Attention Deficit Hyperactivity Disorder (ADHD) is a neurodevelopmental disorder characterised by high levels of inattention, hyperactivity and impulsivity that are present before the age of seven years, seen in a range of situations, inconsistent with the child's developmental level and causing social or academic impairment. Parent training programmes are psychosocial interventions aimed at training parents in techniques to enable them to manage their children's challenging behaviour.
Objectives: To determine whether parent training interventions are effective in reducing ADHD symptoms and associated problems in children aged between five and eigtheen years with a diagnosis of ADHD, compared to controls with no parent training intervention.
Search methods: We searched the following electronic databases (for all available years until September 2010): CENTRAL (2010, Issue 3), MEDLINE (1950 to 10 September 2010), EMBASE (1980 to 2010 Week 36), CINAHL (1937 to 13 September 2010), PsycINFO (1806 to September Week 1 2010), Dissertation Abstracts International (14 September 2010) and the metaRegister of Controlled Trials (14 September 2010). We contacted experts in the field to ask for details of unpublished or ongoing research.
Selection criteria: Randomised (including quasi-randomised) studies comparing parent training with no treatment, a waiting list or treatment as usual (adjunctive or otherwise). We included studies if ADHD was the main focus of the trial and participants were over five years old and had a clinical diagnosis of ADHD or hyperkinetic disorder that was made by a specialist using the operationalised diagnostic criteria of the DSM-III/DSM-IV or ICD-10. We only included trials that reported at least one child outcome.
Data collection and analysis: Four authors were involved in screening abstracts and at least 2 authors looked independently at each one. We reviewed a total of 12,691 studies and assessed five as eligible for inclusion. We extracted data and assessed the risk of bias in the five included trials. Opportunities for meta-analysis were limited and most data that we have reported are based on single studies.
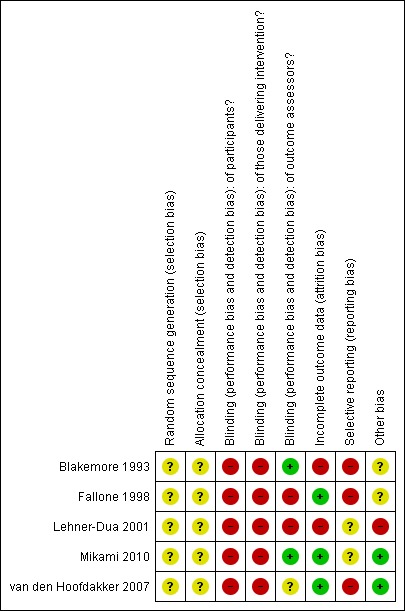
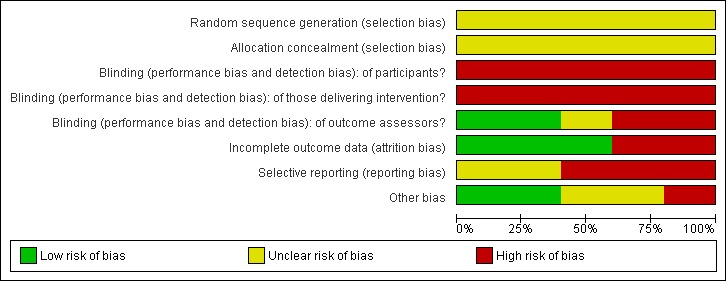
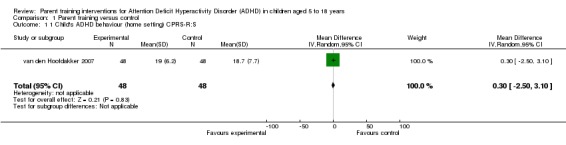
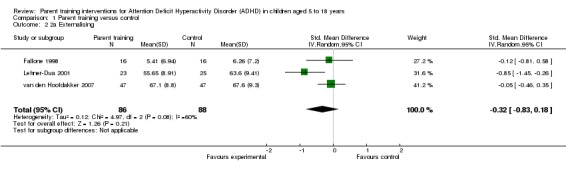
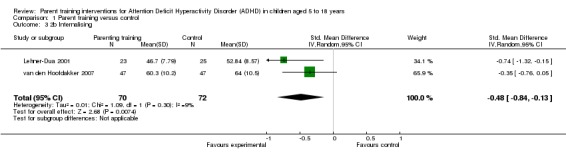
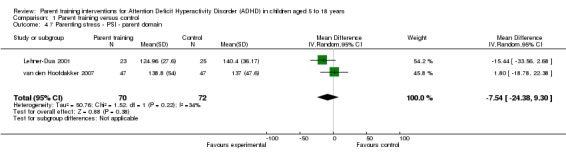
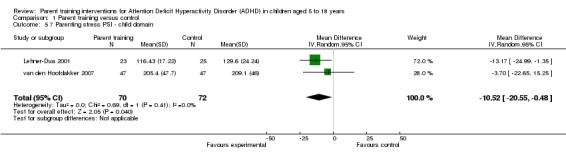
Main results: We found five studies including 284 participants that met the inclusion criteria, all of which compared parent training with de facto treatment as usual (TAU). One study included a nondirective parent support group as a second control arm. Four studies targeted children's behaviour problems and one assessed changes in parenting skills. Of the four studies targeting children's behaviour, two focused on behaviour at home and two focused on behaviour at school. The two studies focusing on behaviour at home had different findings: one found no difference between parent training and treatment as usual, whilst the other reported statistically significant results for parent training versus control. The two studies of behaviour at school also had different findings: one study found no difference between groups, whilst the other reported positive results for parent training when ADHD was not comorbid with oppositional defiant disorder. In this latter study, outcomes were better for girls and for children on medication.We assessed the risk of bias in most of the studies as unclear at best and often as high. Information on randomisation and allocation concealment did not appear in any study report. Inevitably, blinding of participants or personnel was impossible for this intervention; likewise, blinding of outcome assessors (who were most often the parents who had delivered the intervention) was impossible.We were only able to conduct meta-analysis for two outcomes: child 'externalising' behaviour (a measure of rulebreaking, oppositional behaviour or aggression) and child 'internalising' behaviour (for example, withdrawal and anxiety). Meta-analysis of three studies (n = 190) providing data on externalising behaviour produced results that fell short of statistical significance (SMD -0.32; 95% CI -0.83 to 0.18, I(2) = 60%). A meta-analysis of two studies (n = 142) for internalising behaviour gave significant results in the parent training groups (SMD -0.48; 95% CI -0.84 to -0.13, I(2) = 9%). Data from a third study likely to have contributed to this outcome were missing, and we have some concerns about selective outcome reporting bias.Individual study results for child behaviour outcomes were mixed. Positive results on an inventory of child behaviour problems were reported for one small study (n = 24) with the caveat that results were only positive when parent training was delivered to individuals and not groups. In another study (n = 62), positive effects (once results were adjusted for demographic and baseline data) were reported for the intervention group on a social skills measure.The study (n = 48) that assessed parenting skill changes compared parent training with a nondirective parent support group. Statistically significant improvements were reported for the parent training group. Two studies (n = 142) provided data on parent stress indices that were suitable for combining in a meta-analysis. The results were significant for the 'child' domain (MD -10.52; 95% CI -20.55 to -0.48) but not the 'parent' domain (MD -7.54; 95% CI -24.38 to 9.30). Results for this outcome from a small study (n = 24) suggested a long-term benefit for mothers who received the intervention at an individual level; in contrast, fathers benefited from short-term group treatment. A fourth study reported change data for within group measures of parental stress and found significant benefits in only one of the two active parent training group arms (P ≤ 0.01).No study reported data for academic achievement, adverse events or parental understanding of ADHD.
Authors' conclusions: Parent training may have a positive effect on the behaviour of children with ADHD. It may also reduce parental stress and enhance parental confidence. However, the poor methodological quality of the included studies increases the risk of bias in the results. Data concerning ADHD-specific behaviour are ambiguous. For many important outcomes, including school achievement and adverse effects, data are lacking.Evidence from this review is not strong enough to form a basis for clinical practice guidelines. Future research should ensure better reporting of the study procedures and results.
Conflict of interest statement
Morris Zwi ‐ this research was facilitated by the receipt of a PPP Mid‐Career Award which funded a locum 2.5 days per week for one year to allow completion of a diploma in Systematic Reviews methodology at the Systematic Reviews Training Unit, UCL. The Campbell Collaboration contributed £3000 to facilitate the completion of this review. Hannah Jones ‐ none known. Camilla Thorgaard ‐ none known. Ann York ‐ none known. Jane A Dennis ‐ none known.
Figures
Comment in
-
Review: insufficient evidence available on parent training programmes for ADHD in children.Evid Based Ment Health. 2012 Aug;15(3):73. doi: 10.1136/ebmental-2012-100704. Epub 2012 Apr 27. Evid Based Ment Health. 2012. PMID: 22544866 No abstract available.
References
References to studies included in this review
-
- Blakemore B, Shindler S. A problem solving training program for parents of children with attention deficit hyperactivity disorder. Canadian Journal of School Psychology 1993;9(1/Special Issue):66‐85.
-
- Fallone GP. Treatment for Maternal Distress as an Adjunct to Parent‐Training for Children with Attention‐Deficit Hyperactivity Disorder. Memphis TN: University of Memphis, 1998.
-
- Lehner‐Dua LL. The Effectiveness of Russell A Barkley's Parent Training Program on Parents with School‐Aged Children who have ADHD on their Perceived Severity of ADHD, Stress, and Sense of Competence (PhD dissertation). Hempstead, NY: Hofstra University, 2001.
-
- Mikami AY, Jack A, Emeh CC, Stephens HF. Parental influence on children with attention‐deficit/hyperactivity disorder: I. Relationships between parent behaviors and child peer status. Journal of Abnormal Child Psychology 2010;38(6):721‐36. - PMC - PubMed
- Mikami AY, Lerner MD, Griggs MS, McGrath A, Calhoun CD. Parental influence on children with attention‐deficit/hyperactivity disorder: II. Results of a pilot intervention training parents as friendship coaches for children. Journal of Abnormal Child Psychology 2010;38:737‐49. - PMC - PubMed
-
- Hoofdakker BJ, Veen‐Mulders L, Sytema S, Emmelkamp PM, Minderaa RB, Nauta MH. Effectiveness of behavioral parent training for children with ADHD in routine clinical practice: a randomized controlled study. Journal of the American Academy of Child and Adolescent Psychiatry 2007;46(10):1263‐71. - PubMed
References to studies excluded from this review
-
- Abikoff HB, Hechtman L, Klein RG, Gallagher R, Fleiss K, Etcovitch J, et al. Multimodal therapy and stimulants in the treatment of children with attention deficit hyperactivity disorder. Journal of the American Academy of Child and Adolescent Psychiatry 2004;43(7):820‐9. - PubMed
-
- Aman MG, Mcdougle CJ, Scahill L, Handen B, Arnold LE, Johnson C, et al. Medication and parent training in children with pervasive developmental disorders and serious behavior problems: results from a randomized clinical trial. Journal of the American Academy of Child and Adolescent Psychiatry 2009;48(12):1143‐54. - PMC - PubMed
-
- Anastopoulos AD, Shelton TL, DuPaul GJ, Guevremont DC. Parent training for attention‐deficit hyperactivity disorder: its impact on parent functioning. Journal of Abnormal Child Psychology 1993;21(5):581‐96. - PubMed
-
- Arnold SA. Positive Behavior Interventions for Adolescents with ADD/ADHD (Masters' thesis). Long Beach, CA: Callifornia State University, 2007.
-
- Baker‐Ericzen MJ, Hurlburt MS, Brookman‐Frazee L, Jenkins MM, Hough RL. Comparing child, parent, and family characteristics in usual care and empirically supported treatment research samples for children with disruptive behavior disorders. Journal of Emotional and Behavioral Disorders 2010;18(2):82‐99.
Additional references
-
- Abidin RR. Parenting Stress Index. Odessa, FL: Psychological Assessment Resources, Inc, 1986.
-
- Abidin RR. Parenting Stress Index. Revised. Odessa, FL: Psychological Assessment Resources, Inc, 1990.
-
- Abidin RR. Parenting Stress Index. 3rd Edition. Odessa, FL: Psychological Assessment Resources, Inc, 1995.
-
- Achenbach TM, Edelbrock CS. Manual for the Child Behavior Checklist. Burlington, VT: University of Vermont, 1986.
-
- Achenbach TM. Manual for the Child Behavior Checklist /4‐18 and 1991 profile. Burlington, VT: University of Vermont, 1991.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous