

Conservative prevention and management of pelvic organ prolapse in women
- PMID: 22161382
- PMCID: PMC12621084
- DOI: 10.1002/14651858.CD003882.pub4
Conservative prevention and management of pelvic organ prolapse in women
Abstract
Background: Pelvic organ prolapse is common, and some degree of prolapse is seen in 50% of parous women. Women with prolapse can experience a variety of pelvic floor symptoms. Treatments include surgery, mechanical devices and conservative management. Conservative management approaches, such as giving lifestyle advice and delivering pelvic floor muscle training (PFMT), are often used in cases of mild to moderate prolapse. This is an update of a Cochrane review first published in 2004, and previously updated in 2006.
Objectives: To determine the effects of conservative management (physical and lifestyle interventions) for the prevention or treatment of pelvic organ prolapse in comparison with no treatment or other treatment options (such as mechanical devices or surgery).
Search methods: We searched the Cochrane Incontinence Group Specialised Trials Register (searched 6 May 2010), EMBASE (1 January 1996 to 6 May 2010), CINAHL (1 January 1982 to 10 May 2010), PEDro (January 2009), the UK National Research Register (January 2009), ClinicalTrials.gov (April 2009), Current Controlled Trials register (April 2009), CENTRAL (Issue 1, 2009) and ZETOC (January 2009) and the reference lists of relevant articles.
Selection criteria: Randomised and quasi-randomised trials in women with pelvic organ prolapse that included a physical or lifestyle intervention in at least one arm of the trial.
Data collection and analysis: Two reviewers assessed all trials for inclusion/exclusion and methodological quality. Data were extracted by the lead reviewer onto a standard form and cross checked by another. Disagreements were resolved by discussion. Data were processed as described in the Cochrane Handbook for Systematic Reviews of Interventions.
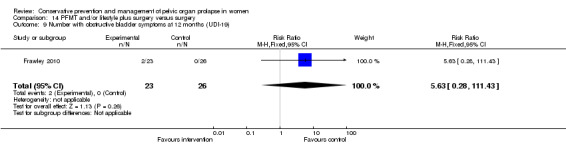
Main results: Six trials were included; three of these trials are new to this update. Four trials were small (less than 25 women per arm) and two had moderate to high risk of bias. Four trials compared PFMT as a treatment for prolapse against a control group (n = 857 women); two trials included women having surgery for prolapse and compared PFMT as an adjunct to surgery versus surgery alone (n = 118 women).PFMT versus controlThere was a significant risk of bias in two out four trials in this comparison. Prolapse symptoms and women's reports of treatment outcomes (primary outcomes) were measured differently in the three trials where this was reported: all three indicated greater improvement in symptoms in the PFMT group compared to the control group. Pooling data on severity of prolapse from two trials indicated that PFMT increases the chance of an improvement in prolapse stage by 17% compared to no PFMT. The two trials which measured pelvic floor muscle function found better function (or improvement in function) in the PFMT group compared to the control group; measurements were not known to be blinded. Two out of three trials which measured urinary outcomes (urodynamics, frequency and bother of symptoms, or symptom score) reported differences between groups in favour of the PFMT group. One trial reported bowel outcomes, showing less frequency and bother with symptoms in the PFMT group compared to the control group.PFMT supplementing surgery versus surgery aloneBoth trials were small and neither measured prolapse-specific outcomes. Pelvic floor muscle function findings differed between the trials: one found no difference between trial groups in muscle strength, whilst the other found a benefit for the PFMT group in terms of stronger muscles. Similarly findings relating to urinary outcomes were contradictory: one trial found no difference in symptom score change between groups, whilst the other found more improvement in urinary symptoms and a reduction in diurnal frequency in the PFMT group compared to the control group.
Authors' conclusions: There is now some evidence available indicating a positive effect of PFMT for prolapse symptoms and severity. The largest most rigorous trial to date suggests that six months of supervised PFMT has benefits in terms of anatomical and symptom improvement (if symptomatic) immediately post-intervention. Further evidence relating to effectiveness and cost-effectiveness of PFMT, of different intensities, for symptomatic prolapse in the medium and long term is needed. A large trial of PFMT supplementing surgery is needed to give clear evidence about the usefulness of combining these treatments. Other comparisons which have not been addressed in trials to date and warrant consideration include those involving lifestyle change interventions, and trials aimed at prolapse prevention.
Conflict of interest statement
Suzanne Hagen was the Chief Investigator of one of the included studies (Hagen 2009), and was one of the reviewers who carried out the study quality assessment and data extraction.
Figures
































Update of
-
Conservative management of pelvic organ prolapse in women.Cochrane Database Syst Rev. 2006 Oct 18;(4):CD003882. doi: 10.1002/14651858.CD003882.pub3. Cochrane Database Syst Rev. 2006. Update in: Cochrane Database Syst Rev. 2011 Dec 07;(12):CD003882. doi: 10.1002/14651858.CD003882.pub4. PMID: 17054190 Updated.
Comment in
-
Pelvic floor muscle training may improve prolapse stage, muscle function and urinary symptoms compared to no training.Evid Based Nurs. 2013 Jan;16(1):7-8. doi: 10.1136/eb-2012-100798. Epub 2012 Sep 13. Evid Based Nurs. 2013. PMID: 22977223 No abstract available.
References
References to studies included in this review
Braekken 2010 {published data only}
-
- Braekken IH, Majida M, Engh ME, Bø K. Morphological changes after pelvic floor muscle training measured by 3‐dimensional ultrasonography: a randomized controlled trial. Obstetrics and Gynaecology 2010;115(2):317‐24. - PubMed
-
- Brækken IH, Majida M, Engh ME, Bø K. Can pelvic floor muscle training reverse pelvic organ prolapse and reduce prolapse symptoms? An assessor‐blinded, randomized, controlled trial. American Journal of Obstetrics and Gynecology 2010;203(2):170e1‐7. - PubMed
Frawley 2010 {published data only}
-
- Frawley HC, Phillips BA, Bø K, Galea MP. Physiotherapy as an adjunct to prolapse surgery: An assessor‐blinded randomized controlled trial. Neurourology and Urodynamics 2010;29:719‐25. - PubMed
Ghroubi 2008 {published data only}
-
- Ghroubi S, Kharrat O, Chaari M, Ben Ayed B, Guermazi M, Elleuch MH. Effect of conservative treatment in the management of low‐degree urogenital prolapse. Annales de réadaptation et de médecine physique 2008;51:96‐102. - PubMed
Hagen 2009 {published and unpublished data}
-
- Hagen S, Stark D, Glazener C, Sinclair L, Ramsay I. A randomised controlled trial of pelvic floor muscle training for stage I and II pelvic organ prolapse. International Urogynecology Journal 2009;20:45‐51. - PubMed
Jarvis 2005 {published data only}
-
- Jarvis SK, Hallam TK, Lujic S, Abbott JA, Vancaillie TG. Peri‐operative physiotherapy improves outcomes for women undergoing incontinence and or prolapse surgery: Results of a randomised controlled trial. Australian and New Zealand Journal of Obstetrics and Gynaecology 2005;45:300‐3. [SR‐INCONT20827] - PubMed
Piya‐Anant 2003 {published data only}
-
- Piya‐Anant M, Therasakvichya S, Leelaphatanadit C, Techatrisak K. Integrated health research program for the Thai elderly: Prevalence of genital prolapse and effectiveness of pelvic floor exercises to prevent worsening of genital prolapse in elderly women. Journal of the Medical Association of Thailand 2003;86:509‐15. - PubMed
References to studies excluded from this review
Adamkiewicz 2001 {published data only}
-
- Adamkiewicz MM, Adamkiewicz MF, Jozwik M, Jozwik M. Combined treatment of pelvic floor exercises and new intravaginal device for genital prolapse. International Urogynaecology Journal. 2001; Vol. 12 (Suppl 3):S48.
Aguirre 2005 {published data only}
-
- Aguirre OA, Davila GW, Lukban JC, Sand PK. Multi‐centre prospective trial of Colpexin® spheres in women with advanced genital prolapse [abstract]. International Urogynecology Journal and Pelvic Floor Dysfunction 2005;16 (Suppl 2):117.
Culligan 2010 {published data only}
-
- Culligan PJ, Scherer J, Dyer K, Priestley JL, Guingon‐White G, Delvecchio D, et al. A randomized clinical trial comparing pelvic floor muscle training to a pilates exercise program for improving pelvic muscle strength. International Urogynecology Journal 2010;21:401‐8. - PubMed
Mimura 2000 {published data only}
-
- Mimura T, Roy AJ, Storrie JB, Kamm MA. Treatment of impaired defecation associated with rectocele by behavioral retraining (biofeedback). Diseases of the Colon and Rectum 2000;43:1267‐72. - PubMed
References to ongoing studies
Barber 2009 {published data only}
Hagen 2010 {unpublished data only}
-
- A multi‐centre randomised controlled trial of a pelvic floor muscle training intervention for women with pelvic organ prolapse (POPPY Trial). Ongoing study April 2007.
Hagen 2011 {published data only}
-
- A Study of the Effects of Physiotherapy to Prevent Pelvic Organ Prolapse (PREVPROL). Ongoing study Recruitment started 12/10/10.
Additional references
Adams 2004
Balmforth 2004
-
- Balmforth J, Bidmead J, et al. Raising the tone: A prospective observational study evaluating the effect of pelvic floor muscle training on bladder neck mobility and associated improvement in stress urinary incontinence. Neurourology and Urodynamics 2004;23(5):553‐4.
Beck 1991
-
- Beck RP, McCormick S, Nordstrom L. A 25‐year experience with 519 anterior colporrhaphy procedures. Obstetrics and Gynecology 1991;78(6):1011‐8. [MEDLINE: ] - PubMed
Bo 2004
-
- Bo K. Pelvic floor muscle training is effective in treatment of female stress urinary incontinence, but how does it work?. International Urogynecology Journal 2004;15:76‐84. - PubMed
Bo 2006
-
- Bo K. Can pelvic floor muscle training prevent and treat pelvic organ prolapse. Acta Obstetrica et Gynecologica 2006;85:263‐8. - PubMed
Bump 1996
-
- Bump RC, Mattiasson A, Bo K, Brubaker LP, DeLancey JO, Klarskov P, et al. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. American Journal of Obstetrics & Gynecology 1996;175(1):10‐7. - PubMed
Bump 1998
-
- Bump R, Norton P. Epidemiology and natural history of pelvic floor dysfunction. Urogynaecology and Pelvic Floor Dysfunction 1998;25(4):723‐46. [MEDLINE: ] - PubMed
Carrière 2006
-
- Carrière B. The pelvic floor. Stuttgard: Georg Thieme Verlag, 2006.
DeLancey 1993
-
- DeLancey JOL. Anatomy and biomechanics of genital prolapse. Clinical Obstetrics and Gynecology 1993;36:897‐909. - PubMed
DeLancey 2007
-
- DeLancey JOL, Morgan DM, Fenner DE, et al. Comparison of levator ani muscle defects and function in women with and without pelvic organ prolapse. Obstetrics and Gynecology 2007;109:295‐302. - PubMed
Dumoulin 2010
Gill 1998
-
- Gill EJ, Hurt WG. Pathophysiology of pelvic organ prolapse. Obstetrics and Gynecology Clinics of North America 1998;25(4):757‐69. [MEDLINE: ] - PubMed
Hagen 2009b
-
- Hagen S, Glazener C, Sinclair L, Stark D, Bugge C. Psychometric properties of the Pelvic Organ Prolapse Symptom Score (POP‐SS). BJOG: an International Journal of Obstetrics and Gynaecology 2009;116:25‐31. - PubMed
Higgins 2009
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. 5.0.2. The Cochrane Collaboration, September 2009.
Hoyte 2001
-
- Hoyte L, Schierlitz L et al. Two and 3‐dimensional MRI comparison of levator ani structure, volume and integrity in women with stress incontinence and prolapsed. Americal Journal of Obstetrics and Gynaecology 2001;185(1):11‐9. - PubMed
Ismail 2010
Kelleher 1997
-
- Kelleher CJ, Cardozo LD, Khullar V, Salvatore S. A new questionnaire to assess the quality of life of urinary incontinent women. British Journal of Obstetrics and Gynaecology 1997;104(12):1374‐9. - PubMed
MacLennan 2000
-
- MacLennan AH, Taylor AW, Wilson DH, Wilson D. The prevalence of pelvic floor muscle disorders and their relationship to gender, age, parity and mode of delivery. British Journal of Obstetrics and Gynaecology 2000;107(12):1460‐70. [MEDLINE: ] - PubMed
Maher 2010
Miller 1998
-
- Miller JM, Ashton‐Miller JA, Delancey J. A pelvic floor muscle precontraction can reduce cough‐related urine loss in selected women with SUI. Journal of the American Geriatric Society 1998;46:870‐4. - PubMed
Morgan 2005
-
- Morgan D M, Gurpeet K, Hsu Y, Fenner D E, Guire K, Miller J, et al. Does vaginal closure force differ in the supine and standing positions?. American Journal of Obstetrics and Gynecology 2005;192:1722‐8. - PubMed
Mouritsen 2003
-
- Mouritsen L, Larsen JP. Symptoms, bother and POP‐Q in women referred with pelvic organ prolapse. International Urogynecology Journal of Pelvic Floor Dysfunction 2003;14:122‐7. - PubMed
Olsen 1997
-
- Olsen AL, Smith VJ, Bergstrom JO, Colling JC, Clark AL. Epidemiology of surgically managed pelvic organ and urinary incontinence. Obstetrics and Gynecology 1997;89(4):501‐6. [MEDLINE: ] - PubMed
Peschers 2001
-
- Peschers U, Fanger G, Schaer G, Vodusek D, Delancey J, Schussler B. Bladder neck mobility in continent nulliparous women. British Journal of Obstetrics & Gynaecology 2001;108:320‐4. - PubMed
Poma 2000
-
- Poma P. Nonsurgical Management of Genital Prolapse. Journal of Reproductive Medicine 2000;45(10):789‐97. [MEDLINE: ] - PubMed
Slieker‐ten Hove 2004
-
- Slieker‐ten Hove MCP, Vierhout M, Bloembergan H, Schoenmaker G. Distribution of pelvic organ prolapse (POP) in the general population: prevalence, severity, etiology and relation with the function of the pelvic floor muscles. International Continence Society, 34th Annual Meeting; 2004 Aug 25‐27; Paris, France. 2004.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous